

Prognostic value of skeletal muscle mass during tyrosine kinase inhibitor (TKI) therapy in cancer patients: a systematic review and meta-analysis
- PMID: 33337518
- PMCID: PMC8310498
- DOI: 10.1007/s11739-020-02589-5
Prognostic value of skeletal muscle mass during tyrosine kinase inhibitor (TKI) therapy in cancer patients: a systematic review and meta-analysis
Abstract
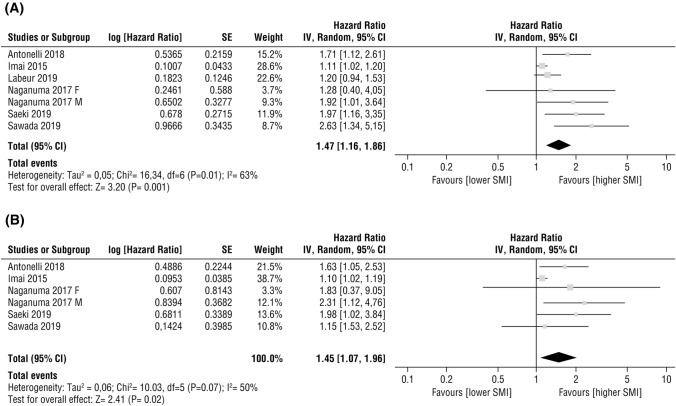
Low muscle mass has been associated with worse clinical outcomes in various cancers. This work investigated whether, during tyrosine kinases inhibitors (TKIs) therapy, low muscle mass was associated with treatment toxicity and survival outcomes. A systematic literature search was performed in Pubmed, Web of Science, and Scopus databases from inception to June 2020, based on fixed inclusion and exclusion criteria. Effect sizes were estimated with hazard ratios (HR) and odds ratios (OR) with 95% confidence interval (CI) and heterogeneity was assessed by measuring inconsistency (I2) based on the Chi squared test. A total of 24 retrospective studies were identified, enrolling patients treated with sorafenib (n = 12), sunitinib (n = 6), lenvatinib (n = 3), regorafenib (n = 2), gefitinib (n = 1), imatinib (n = 1), and pazopanib (n = 1). Thirteen studies were deemed eligible for pooled analyses. Meta-analyses found a significant effect of low muscle mass on dose-limiting toxicity (DLT) (OR 2.40, 95% CI 1.26-4.58, p = 0.008, I2 = 51%) in patients treated with TKI therapy. A subgroup analysis by treatment showed an association between DLT and low muscle during sorafenib or sunitinib, although not significant. A significant association between low skeletal muscle index and poorer overall survival was observed in HCC patients treated with sorafenib (HR 1.45, 95% CI 1.07-1.96, p = 0.02). For other TKIs, although some results showed an association between low muscle mass and worse outcomes, the number of studies for each TKI therapy was too small to reach conclusions. Skeletal muscle mass could influence the prognosis of some TKI-treated patients. This effect is demonstrated in sorafenib-treated HCC patients but remains almost unexplored in other cancer patients undergoing TKI therapy. Further prospective studies with large sample size and sufficient follow-up are needed to clarify the role of muscle mass in the metabolism of TKI-based cancer treatment, and its association with toxicity and survival.
Keywords: Chemotherapy toxicity; L3 skeletal muscle index; Personalized medicine; Skeletal muscle mass; Survival; Tyrosine kinase inhibitors.
© 2020. The Author(s).
Conflict of interest statement
All the authors declare that they have no conflicts of interest that might be relevant to the contents of this article.
Figures


References
-
- Park I, Choi SJ, Kim YS, Ahn HK, Hong J, Sym SJ, et al. Prognostic factors for risk stratification of patients with recurrent or metastatic pancreatic adenocarcinoma who were treated with gemcitabine-based chemotherapy. Cancer Res Treat. 2016;48:1264–1273. doi: 10.4143/crt.2015.250. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
