

Burosumab for the Treatment of Tumor-Induced Osteomalacia
- PMID: 33338281
- PMCID: PMC8247961
- DOI: 10.1002/jbmr.4233
Burosumab for the Treatment of Tumor-Induced Osteomalacia
Abstract
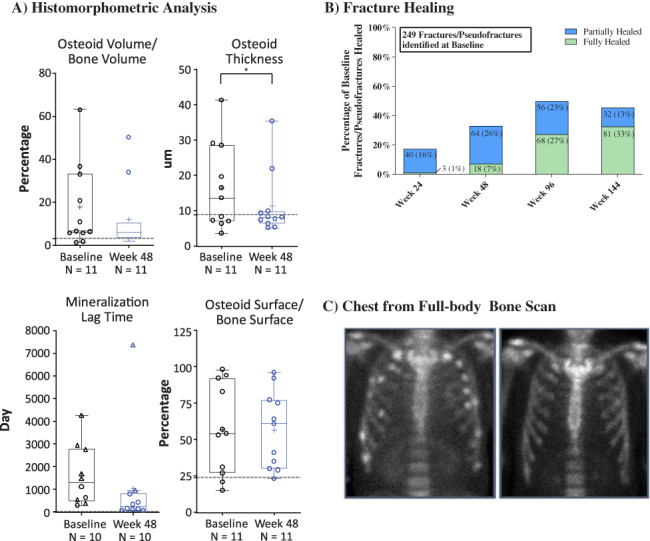
Tumor-induced osteomalacia (TIO) is caused by phosphaturic mesenchymal tumors producing fibroblast growth factor 23 (FGF23) and is characterized by impaired phosphate metabolism, skeletal health, and quality of life. UX023T-CL201 is an ongoing, open-label, phase 2 study investigating the safety and efficacy of burosumab, a fully human monoclonal antibody that inhibits FGF23, in adults with TIO or cutaneous skeletal hypophosphatemia syndrome (CSHS). Key endpoints were changes in serum phosphorus and osteomalacia assessed by transiliac bone biopsies at week 48. This report focuses on 14 patients with TIO, excluding two diagnosed with X-linked hypophosphatemia post-enrollment and one with CSHS. Serum phosphorus increased from baseline (0.52 mmol/L) and was maintained after dose titration from week 22 (0.91 mmol/L) to week 144 (0.82 mmol/L, p < 0.0001). Most measures of osteomalacia were improved at week 48: osteoid volume/bone, osteoid thickness, and mineralization lag time decreased; osteoid surface/bone surface showed no change. Of 249 fractures/pseudofractures detected across 14 patients at baseline, 33% were fully healed and 13% were partially healed at week 144. Patients reported a reduction in pain and fatigue and an increase in physical health. Two patients discontinued: one to treat an adverse event (AE) of neoplasm progression and one failed to meet dosing criteria (receiving minimal burosumab). Sixteen serious AEs occurred in seven patients, and there was one death; all serious AEs were considered unrelated to treatment. Nine patients had 16 treatment-related AEs; all were mild to moderate in severity. In adults with TIO, burosumab exhibited an acceptable safety profile and was associated with improvements in phosphate metabolism and osteomalacia. © 2020 The Authors. Journal of Bone and Mineral Research published by American Society for Bone and Mineral Research..
Keywords: BONE HISTOMORPHOMETRY; CLINICAL TRIALS; OSTEOMALACIA AND RICKETS; PTH/VIT D/FGF23; TUMOR-INDUCED BONE DISEASE.
© 2020 The Authors. Journal of Bone and Mineral Research published by American Society for Bone and Mineral Research.
Figures

Comment in
-
Tumor-Induced Osteomalacia: Treatment Progress Using Burosumab, an Anti-FGF23 Monoclonal Antibody.J Bone Miner Res. 2021 Apr;36(4):625-626. doi: 10.1002/jbmr.4280. Epub 2021 Mar 19. J Bone Miner Res. 2021. PMID: 33740291 No abstract available.
-
Burosumab for Tumor-Induced Osteomalacia: Not Enough of a Good Thing.J Bone Miner Res. 2021 Dec;36(12):2453-2454. doi: 10.1002/jbmr.4318. Epub 2021 May 5. J Bone Miner Res. 2021. PMID: 33950530 No abstract available.
-
Reply to: Burosumab for Tumor-Induced Osteomalacia: not Enough of a Good Thing.J Bone Miner Res. 2021 Dec;36(12):2455-2456. doi: 10.1002/jbmr.4317. Epub 2021 May 24. J Bone Miner Res. 2021. PMID: 34030212 Free PMC article. No abstract available.
References
-
- Minisola S, Peacock M, Fukumoto S, et al. Tumour‐induced osteomalacia. Nat Rev Dis Primers. 2017;3:17044. - PubMed
-
- Imel EA, Peacock M, Pitukcheewanont P, et al. Sensitivity of fibroblast growth factor 23 measurements in tumor‐induced osteomalacia. J Clin Endocrinol Metab. 2006;91(6):2055–61. - PubMed
-
- Lamb YN. Burosumab: first global approval. Drugs. 2018;78(6):707–714. - PubMed
-
- Whyte MP, Carpenter TO , Gottesman GS, et al. Efficacy and safety of burosumab in children aged 1–4 years with X‐linked hypophosphataemia: a multicentre, open‐label, phase 2 trial. Lancet Diabetes Endocrinol. 2019;7(3):189–99. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
