

Neuroimaging manifestations in children with SARS-CoV-2 infection: a multinational, multicentre collaborative study
- PMID: 33338439
- PMCID: PMC7744016
- DOI: 10.1016/S2352-4642(20)30362-X
Neuroimaging manifestations in children with SARS-CoV-2 infection: a multinational, multicentre collaborative study
Abstract
Background: The CNS manifestations of COVID-19 in children have primarily been described in case reports, which limit the ability to appreciate the full spectrum of the disease in paediatric patients. We aimed to identify enough cases that could be evaluated in aggregate to better understand the neuroimaging manifestations of COVID-19 in the paediatric population.
Methods: An international call for cases of children with encephalopathy related to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection and abnormal neuroimaging findings was made. Clinical history and associated plasma and cerebrospinal fluid data were requested. These data were reviewed by a central neuroradiology panel, a child neurologist, and a paediatric infectious diseases expert. The children were categorised on the basis of their time of probable exposure to SARS-CoV-2. In addition, cases were excluded when a direct link to SARS-CoV-2 infection could not be established or an established alternate diagnostic cause could be hypothesised. The accepted referral centre imaging data, from ten countries, were remotely reviewed by a central panel of five paediatric neuroradiologists and a consensus opinion obtained on the imaging findings.
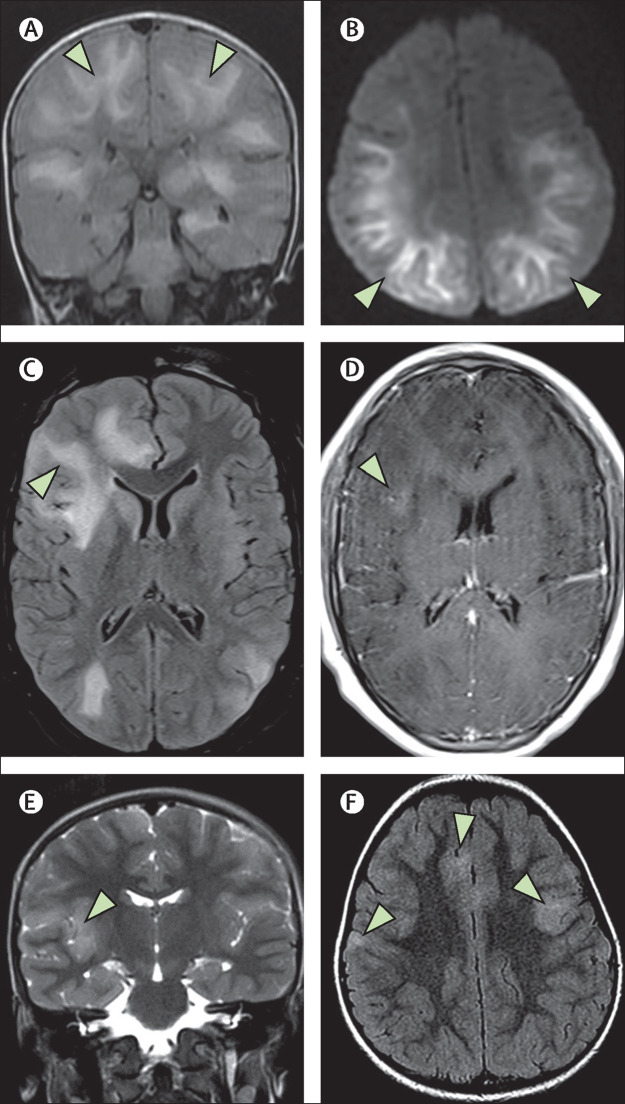
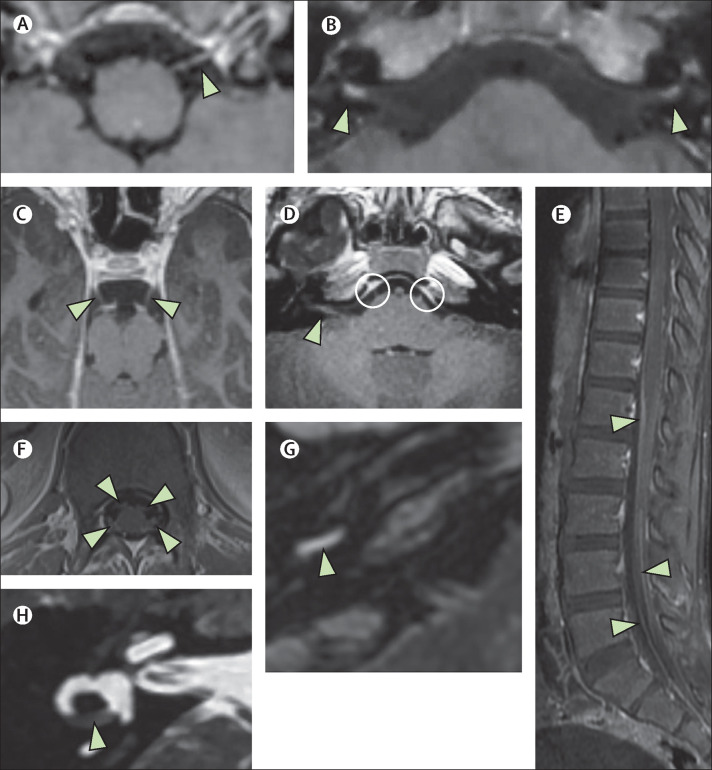
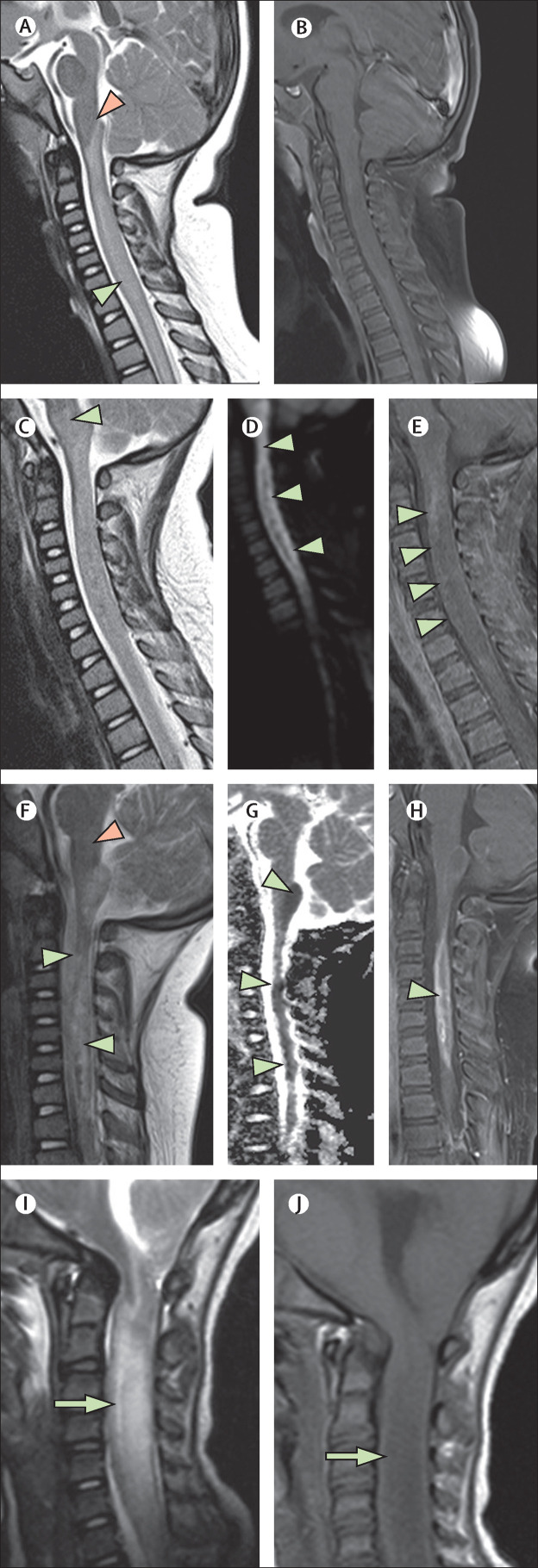
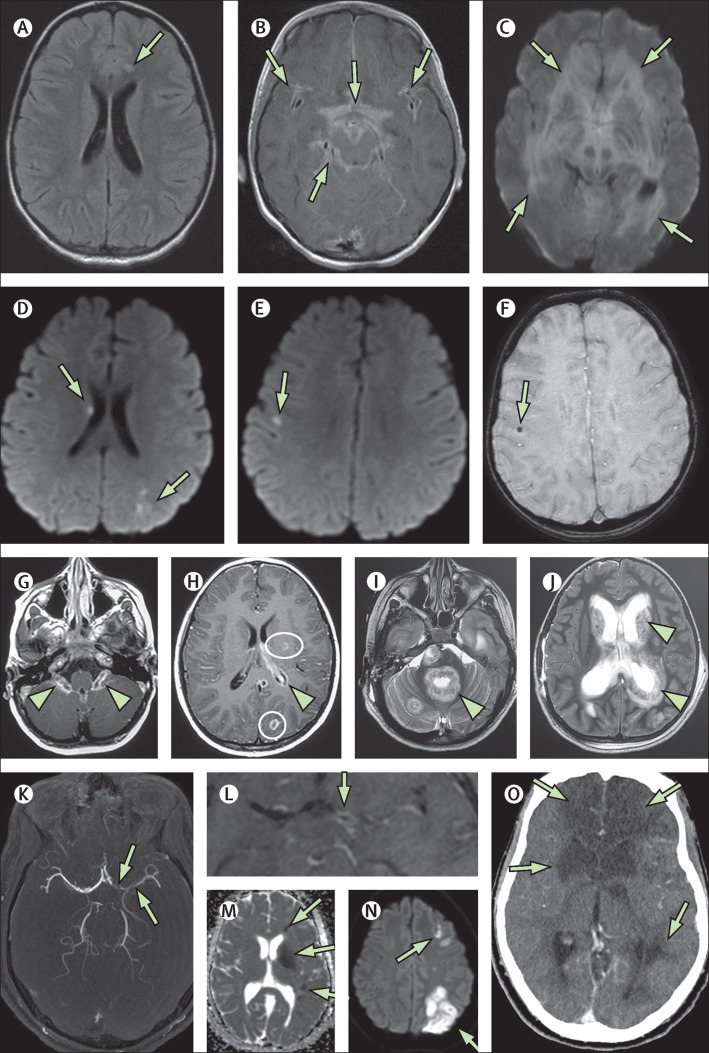
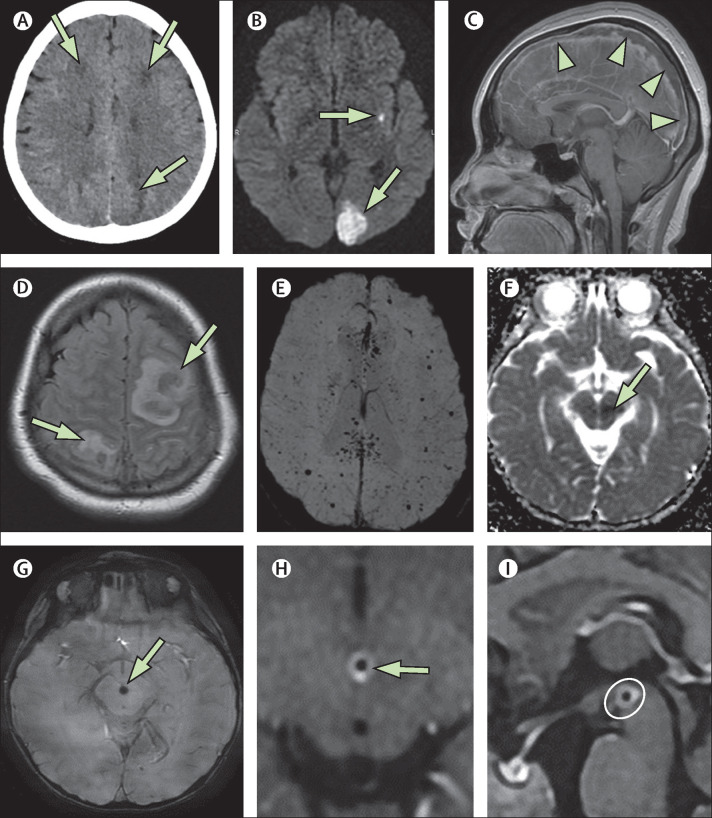
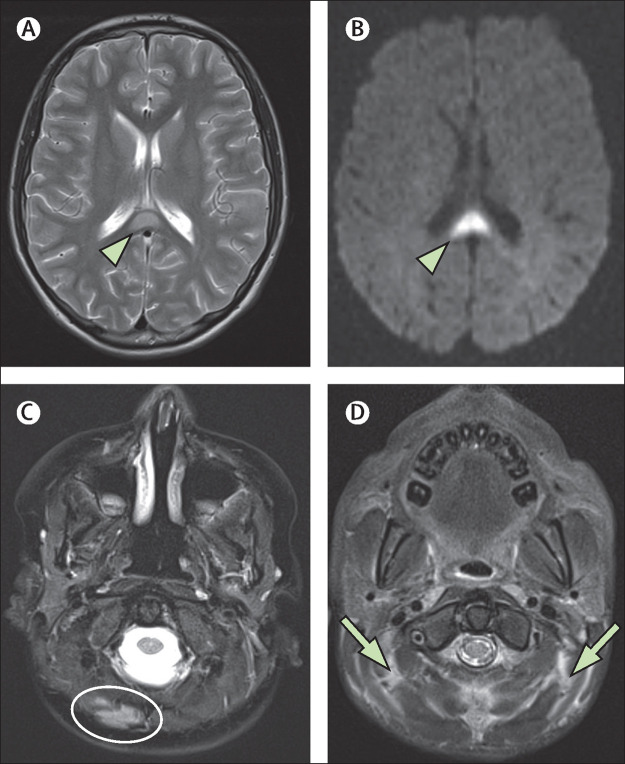
Findings: 38 children with neurological disease related to SARS-CoV-2 infection were identified from France (n=13), the UK (n=8), the USA (n=5), Brazil (n=4), Argentina (n=4), India (n=2), Peru (n=1), and Saudi Arabia (n=1). Recurring patterns of disease were identified, with neuroimaging abnormalities ranging from mild to severe. The most common imaging patterns were postinfectious immune-mediated acute disseminated encephalomyelitis-like changes of the brain (16 patients), myelitis (eight patients), and neural enhancement (13 patients). Cranial nerve enhancement could occur in the absence of corresponding neurological symptoms. Splenial lesions (seven patients) and myositis (four patients) were predominantly observed in children with multisystem inflammatory syndrome. Cerebrovascular complications in children were less common than in adults. Significant pre-existing conditions were absent and most children had favourable outcomes. However, fatal atypical CNS co-infections developed in four previously healthy children infected with SARS-CoV-2.
Interpretation: Acute-phase and delayed-phase SARS-CoV-2-related CNS abnormalities are seen in children. Recurring patterns of disease and atypical neuroimaging manifestations can be found and should be recognised being as potentially due to SARS-CoV-2 infection as an underlying aetiological factor. Studies of paediatric specific cohorts are needed to better understand the effects of SARS-CoV-2 infection on the CNS at presentation and on long-term follow-up in children.
Funding: American Society of Pediatric Neuroradiology, University of Manchester (Manchester, UK). VIDEO ABSTRACT.
Copyright © 2021 Elsevier Ltd. All rights reserved.
Figures
References
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
