A multicenter observational study on Medication-Related Osteonecrosis of the Jaw (MRONJ) in advanced cancer and myeloma patients of a cancer network in North-Western Italy
- PMID: 33340073
- PMCID: PMC8254890
- DOI: 10.4317/medoral.24318
A multicenter observational study on Medication-Related Osteonecrosis of the Jaw (MRONJ) in advanced cancer and myeloma patients of a cancer network in North-Western Italy
Abstract
Background: Incidence of Medication-Related Osteonecrosis of the Jaw (MRONJ) related to cancer and myeloma treatments is undetermined, with scarce data varying from 2 to 7.8/million/year in limited investigated populations. A 9-years [2009-2018] regional-wide survey was conducted, deploying the North-Western Italy Cancer Network ("Rete Oncologica Piemonte e Valle d'Aosta"), to assess number and main characteristics of MRONJ cases among myeloma/cancer patients, within a population of 4.5 million inhabitants.
Material and methods: MRONJ cases were collected retrospectively from January 2009 to June 2015; from July 2015 to December 2018, data were collected prospectively. Number of new MRONJ cases per year, underlying disorder, drug(s) administered, treatment duration, site and onset timing of MRONJ were detailed.
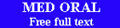
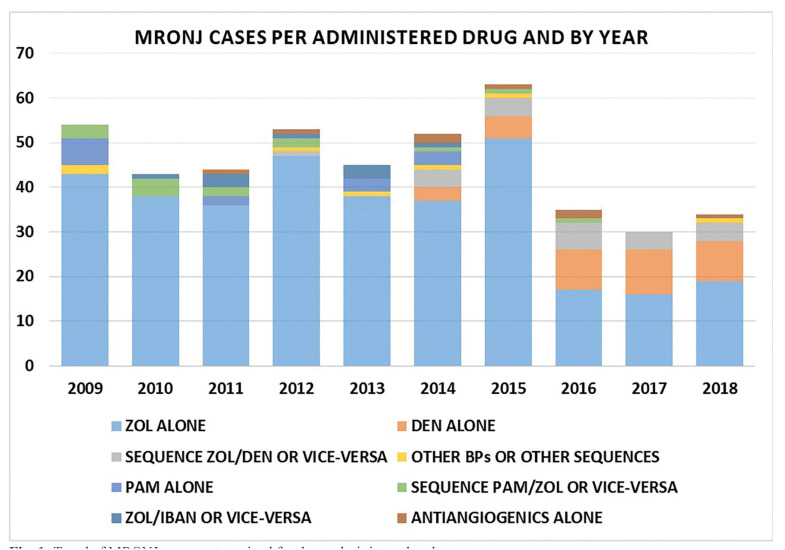
Results: 459 MRONJ cases were identified. Primary diseases were breast cancer (46%), prostate cancer (21%), myeloma (19%), and other types of carcinoma (14%). Patients received antiresorptive treatment either alone (399; 88.47%) or in combination with biological agents (52; 11.53%); 8 patients (1.7%) received only antiangiogenic drugs. Zoledronic acid [388] and denosumab [59] were the most frequently administered drugs. Mandible was involved in 296 (64,5%) cases. Number of new MRONJ cases was stable from 2009 to 2015, with a mean of 51.3 cases per year (raw incidence: 11.6/million/year), declining in the 2016-2018 years to 33.3 cases per year (raw incidence: 7.5/million/year).
Conclusions: With such discrepancy of cases overtime being partially explicable, number of new MRONJ cases per year are consistent with those observed in a previous study [2003-2008] in the same region, being instead higher than those reported in other populations.
Conflict of interest statement
Conflicts of interest Dr. Vittorio reports financial relationship in the form of travel grants provided by from Kyowa Kirin, and Celgene, outside the submitted work. Dr. Alessio Gambino reports financial relationship in the form of a grant from North-Western Italy Cancer Network (“Rete Oncologica Piemonte e Valle d’Aosta”).
Figures
References
-
- Ruggiero SL, Dodson TB, Fantasia J, Goodday R, Aghaloo T, Mehrotra B. American Association of Oral and Maxillofacial Surgeons position paper on medication-related osteonecrosis of the jaw--2014 update. J Oral Maxillofac Surg. 2014;72:1938–56. - PubMed
-
- Otto S, Marx RE, Tröltzsch M, Ristow O, Ziebart T, Al-Nawas B. Comments on "diagnosis and management of osteonecrosis of the jaw: a systematic review and international consensus". J Bone Miner Res. 2015;30:1113–15. - PubMed
-
- Fusco V, Bedogni A, Addeo A, Campisi G. Definition and estimation of osteonecrosis of jaw (ONJ), and optimal duration of antiresorptive treatment in bone metastatic cancer patients: supplementary data from the denosumab extension study? Support Care Cancer. 2017;25:345–49. - PubMed
-
- Solomon DH, Mercer E, Woo SB, Avorn J, Schneeweiss S, Treister N. Defining the epidemiology of bisphosphonate-associated osteonecrosis of the jaw: prior work and current challenges. Osteoporos Int. 2013;24:237–44. - PubMed