

APOE and Alzheimer's disease: advances in genetics, pathophysiology, and therapeutic approaches
- PMID: 33340485
- PMCID: PMC8096522
- DOI: 10.1016/S1474-4422(20)30412-9
APOE and Alzheimer's disease: advances in genetics, pathophysiology, and therapeutic approaches
Erratum in
-
Correction to Lancet Neurol 2021; 20: 68-80.Lancet Neurol. 2021 Feb;20(2):e2. doi: 10.1016/S1474-4422(21)00004-1. Epub 2021 Jan 20. Lancet Neurol. 2021. PMID: 33484655 No abstract available.
Abstract
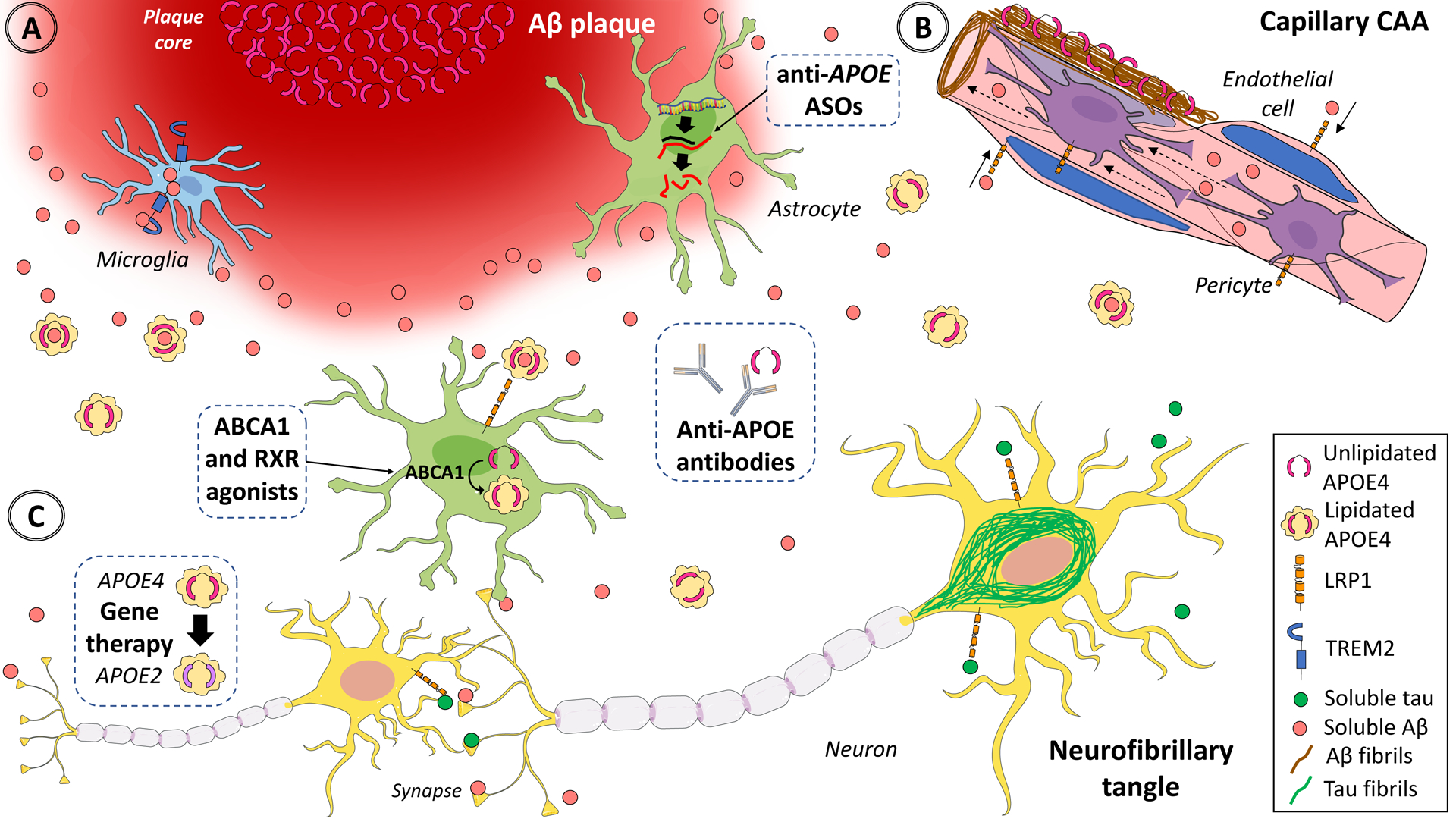
The APOE ε4 allele remains the strongest genetic risk factor for sporadic Alzheimer's disease and the APOE ε2 allele the strongest genetic protective factor after multiple large scale genome-wide association studies and genome-wide association meta-analyses. However, no therapies directed at APOE are currently available. Although initial studies causally linked APOE with amyloid-β peptide aggregation and clearance, over the past 5 years our understanding of APOE pathogenesis has expanded beyond amyloid-β peptide-centric mechanisms to tau neurofibrillary degeneration, microglia and astrocyte responses, and blood-brain barrier disruption. Because all these pathological processes can potentially contribute to cognitive impairment, it is important to use this new knowledge to develop therapies directed at APOE. Several therapeutic approaches have been successful in mouse models expressing human APOE alleles, including increasing or reducing APOE levels, enhancing its lipidation, blocking the interactions between APOE and amyloid-β peptide, and genetically switching APOE4 to APOE3 or APOE2 isoforms, but translation to human clinical trials has proven challenging.
Copyright © 2021 Elsevier Ltd. All rights reserved.
Figures
References
-
- Belloy ME, Napolioni V, Han SS, Le Guen Y, Greicius MD, Alzheimer’s Disease Neuroimaging Initiative. Association of Klotho-VS Heterozygosity With Risk of Alzheimer Disease in Individuals Who Carry APOE4. JAMA Neurol 2020; published online April 13. DOI: 10.1001/jamaneurol.2020.0414. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
