

Effects of variations in access to care for children with atopic dermatitis
- PMID: 33341118
- PMCID: PMC7749983
- DOI: 10.1186/s12895-020-00114-x
Effects of variations in access to care for children with atopic dermatitis
Abstract
Background: An estimated 50% of children in the US are Medicaid-insured. Some of these patients have poor health literacy and limited access to medications and specialty care. These factors affect treatment utilization for pediatric patients with atopic dermatitis (AD), the most common inflammatory skin disease in children. This study assesses and compares treatment patterns and healthcare resource utilization (HCRU) between large cohorts of Medicaid and commercially insured children with AD.
Methods: Pediatric patients with AD were identified from 2 large US healthcare claims databases (2011-2016). Included patients had continuous health plan eligibility for ≥6 months before and ≥12 months after the first AD diagnosis (index date). Patients with an autoimmune disease diagnosis within 6 months of the index date were excluded. Treatment patterns and all-cause and AD-related HCRU during the observation period were compared between commercially and Medicaid-insured children.
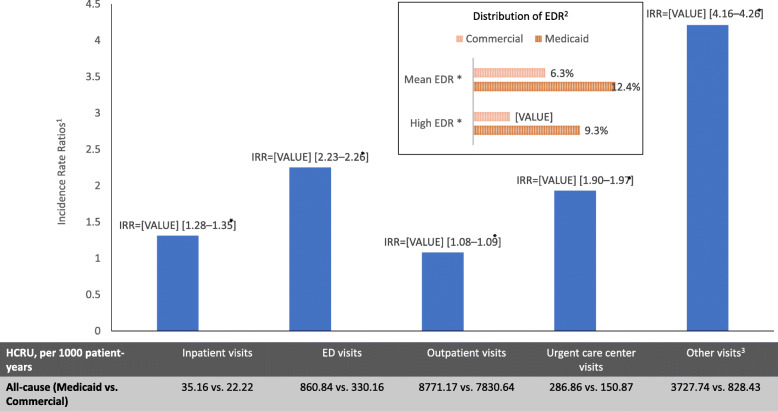
Results: A minority of children were evaluated by a dermatology or allergy/immunology specialist. Several significant differences were observed between commercially and Medicaid-insured children with AD. Disparities detected for Medicaid-insured children included: comparatively fewer received specialist care, emergency department and urgent care center utilization was higher, a greater proportion had asthma and non-atopic morbidities, high- potency topical corticosteroids and calcineurin inhibitors were less often prescribed, and prescriptions for antihistamines were more than three times higher, despite similar rates of comorbid asthma and allergies among antihistamine users. Treatment patterns also varied substantially across physician specialties.
Conclusions: Results suggest barriers in accessing specialty care for all children with AD and significant differences in management between commercially and Medicaid-insured children. These disparities in treatment and access to specialty care may contribute to poor AD control, especially in Medicaid-insured patients.
Keywords: Access to care; Atopic dermatitis; Atopic eczema; Children; Emergency department reliance; Medicaid; Private insurance.
Conflict of interest statement
This study was funded by Regeneron Pharmaceuticals, Inc. and Sanofi. A. Gadkari was an employee and stockholder in Regeneron Pharmaceuticals Inc. at the time the study was conducted. P. Mina-Osorio was an employee of and stockholder in Regeneron Pharmaceuticals Inc. at the time of the study M. Kaur, U. Mallya, and R. Miao are employees and stockholder in Sanofi. F. Vekeman and J. Héroux are employees of StatLog Inc., which received research funding for the current study. A. S. Paller is an employee of Northwestern University. She has been a consultant with honorarium for Regeneron Pharmaceuticals and Sanofi and investigator for Regeneron Pharmaceuticals. E. C. Siegfried is an employee of Saint-Louis University. She has been a consultant with honorarium and an investigator for Regeneron Pharmaceuticals and Sanofi.
Figures
Similar articles
-
Examining racial and ethnic disparities in diagnosis and access to care in infantile atopic dermatitis in the USA: a retrospective cohort study.Br J Dermatol. 2024 Dec 23;192(1):144-151. doi: 10.1093/bjd/ljae322. Br J Dermatol. 2024. PMID: 39163520
-
Burden of illness in patients with possible Lennox-Gastaut syndrome: A retrospective claims-based study.Epilepsy Behav. 2018 Nov;88:66-73. doi: 10.1016/j.yebeh.2018.08.032. Epub 2018 Sep 18. Epilepsy Behav. 2018. PMID: 30241056
-
Lack of financial barriers to pediatric cochlear implantation: impact of socioeconomic status on access and outcomes.Arch Otolaryngol Head Neck Surg. 2010 Jul;136(7):648-57. doi: 10.1001/archoto.2010.90. Arch Otolaryngol Head Neck Surg. 2010. PMID: 20644058
-
Atopic Dermatitis: The Role of the Social Determinants of Health on Severity and Access to Care.Dermatol Clin. 2024 Oct;42(4):635-638. doi: 10.1016/j.det.2024.06.003. Epub 2024 Jul 24. Dermatol Clin. 2024. PMID: 39278717 Review.
-
Trends in private insurance, Medicaid/State Children's Health Insurance Program, and the health-care safety net: implications for asthma disparities.Chest. 2007 Nov;132(5 Suppl):818S-830S. doi: 10.1378/chest.07-1903. Chest. 2007. PMID: 17998346 Review.
Cited by
-
Systemic Therapy for Atopic Dermatitis in Children and Adolescents: A US Expert Consensus.Dermatology. 2024;240(5-6):897-909. doi: 10.1159/000540920. Epub 2024 Oct 15. Dermatology. 2024. PMID: 39406204 Free PMC article.
-
Managing Childhood and Adolescent Atopic Dermatitis in Primary Care: A US Expert Group Consensus.J Pediatr Clin Pract. 2024 Jul 10;14:200121. doi: 10.1016/j.jpedcp.2024.200121. eCollection 2024 Dec. J Pediatr Clin Pract. 2024. PMID: 39950052 Free PMC article.
-
Reframing racial and ethnic disparities in atopic dermatitis in Black and Latinx populations.J Allergy Clin Immunol. 2021 Nov;148(5):1104-1111. doi: 10.1016/j.jaci.2021.09.015. Epub 2021 Sep 30. J Allergy Clin Immunol. 2021. PMID: 34600773 Free PMC article. Review.
-
The reporting of social determinants of health in pediatric dermatology clinical trials: a systematic review.Int J Womens Dermatol. 2024 Aug 19;10(3):e173. doi: 10.1097/JW9.0000000000000173. eCollection 2024 Oct. Int J Womens Dermatol. 2024. PMID: 39161756 Free PMC article.
-
Pharmacoequity in Allergy-Immunology: Disparities in Access to Medications for Allergic Diseases and Proposed Solutions in the United States and Globally.J Allergy Clin Immunol Pract. 2024 Feb;12(2):272-280. doi: 10.1016/j.jaip.2023.11.005. Epub 2023 Nov 10. J Allergy Clin Immunol Pract. 2024. PMID: 37951413 Free PMC article. Review.
References
-
- Centers for Medicare & Medicaid Services . FFY 2018 Number of Children Ever-Enrolled in Medicaid and CHIP. Statistical Enrollment Data System. 2018.
-
- United States Census Bureau . QuickFacts United States. 2018.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
