

Dolutegravir in pregnant mice is associated with increased rates of fetal defects at therapeutic but not at supratherapeutic levels
- PMID: 33341441
- PMCID: PMC7753150
- DOI: 10.1016/j.ebiom.2020.103167
Dolutegravir in pregnant mice is associated with increased rates of fetal defects at therapeutic but not at supratherapeutic levels
Abstract
Background: Dolutegravir (DTG) is a preferred regimen for all people with HIV including pregnant women, but its effects on the fetus are not fully understood. Periconceptional exposure to DTG has been associated with increased rates of neural tube defects (NTDs), although it is unknown whether this is a causal relationship. This has led to uncertainty around the use of DTG in women of reproductive potential.
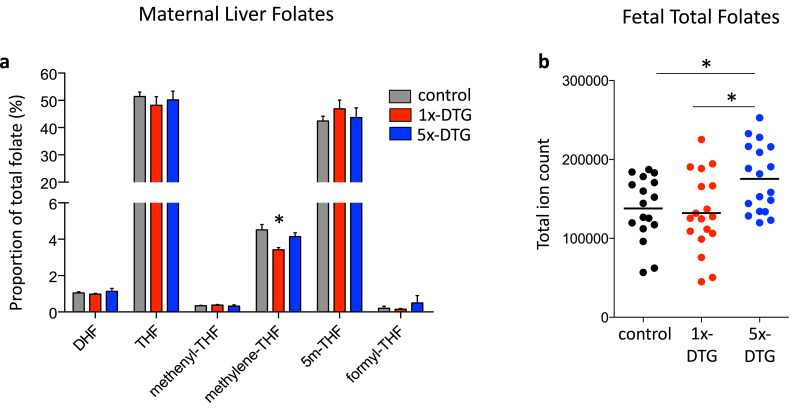
Methods: Pregnant C57BL/6J mice were randomly allocated to control (water), 1x-DTG (2.5 mg/kg-peak plasma concentration ~3000 ng/ml - therapeutic level), or 5x-DTG (12.5 mg/kg-peak plasma concentration ~12,000 ng/ml - supratherapeutic level), once daily from gestational day 0.5 until sacrifice. DTG was administered with 50 mg/kg tenofovir+33.3 mg/kg emtricitabine. Fetal phenotypes were determined, and maternal and fetal folate levels were quantified by mass-spectrometry.
Findings: 352 litters (91 control, 150 1x-DTG, 111 5x-DTG) yielding 2776 fetuses (747 control, 1174 1x-DTG, 855 5x-DTG) were assessed. Litter size and viability rates were similar between groups. Fetal and placenta weights were lower in the 1x-DTG vs. control. Placental weight was higher in the 5x-DTG vs. control. Five NTDs were observed, all in the 1x-DTG group. Fetal defects, including microphthalmia, severe edema, and vascular/bleeding defects were more frequent in the 1x-DTG group. In contrast, defect rates in the 5x-DTG were similar to control. Fetal folate levels were similar between control and 1x-DTG, but were significantly higher in the 5x-DTG group.
Interpretation: Our findings support a causal relationship of DTG at therapeutic doses with increased risk for fetal defects, including NTDs at a rate that is similar that reported in the Tsepamo study for women exposed to DTG-based ART from conception. The non-monotonic dose-response relationship between DTG and fetal anomalies could explain the previous lack of fetal toxicity findings from pre-clinical DTG studies. The fetal folate levels suggest that DTG is unlikely to be an inhibitor of folate uptake.
Funding: This project has been funded with Federal funds from the Eunice Kennedy Shriver National Institute of Child Health and Human Development, National Institutes of Health, Department of Health and Human Services, under Contract No. HHSN275201800001I.
Copyright © 2020 The Authors. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest The authors have no competing interests relating to this study. AJC acts as consultant for ViiV Healthcare Limited, with any fees going to support his research program. LS received personal support for participating in a ViiV organized Think Tank.
Figures





Comment in
-
Letter to the editor in re: Mohan et al., 2020 'dolutegravir in pregnant mice is associated with increased rates of fetal defects at therapeutic but not at supratherapeutic levels'.EBioMedicine. 2021 Apr;66:103335. doi: 10.1016/j.ebiom.2021.103335. Epub 2021 Apr 12. EBioMedicine. 2021. PMID: 33857900 Free PMC article. No abstract available.
References
-
- Vitoria M. The transition to dolutegravir and other new antiretrovirals in low-income and middle-income countries: what are the issues? AIDS. 2018;32:1551–1561. - PubMed
-
- World Health Organization Consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection . 2nd ed. 2016. Recommendations for a Public Health Approach.www.who.int/hiv/pub/arv/arv-2016/en Available at: - PubMed
-
- R. Zash R. IAS Virtual; Botswana: 2020. Update on Neural Tube Defects With Antiretroviral Exposure in the Tsepamo Study. abstract OAXLB0102.
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
