

Clinical and Laboratory Aspects of Insulin Autoantibody-Mediated Glycaemic Dysregulation and Hyperinsulinaemic Hypoglycaemia: Insulin Autoimmune Syndrome and Exogenous Insulin Antibody Syndrome
- PMID: 33343044
- PMCID: PMC7731936
- DOI: 10.33176/AACB-20-00008
Clinical and Laboratory Aspects of Insulin Autoantibody-Mediated Glycaemic Dysregulation and Hyperinsulinaemic Hypoglycaemia: Insulin Autoimmune Syndrome and Exogenous Insulin Antibody Syndrome
Abstract
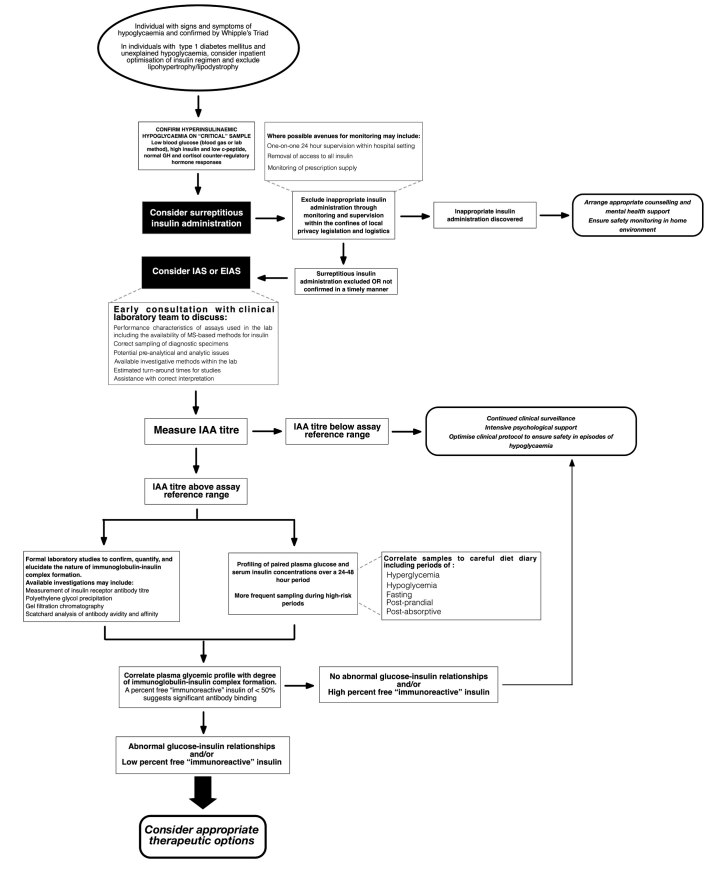
Autoimmune glycaemic dysregulation and hyperinsulinaemic hypoglycaemia mediated by insulin autoantibodies is an increasingly recognised but controversial phenomenon described in both exogenous insulin naïve (insulin autoimmune syndrome) and exposed (exogenous insulin antibody syndrome) individuals. There has been a significant proliferation of case reports, clinical studies and reviews in the medical literature in recent years which have collectively highlighted the discrepancy between experts in the field with regard to the nomenclature, definition, proposed pathophysiology, as well as the clinical and biochemical diagnostic criteria associated with the condition. The essential characteristics of the condition are glycaemic dysregulation manifesting as episodes of hyperglycaemia and unpredictable hyperinsulinaemic hypoglycaemia associated with high titres of endogenous antibodies to insulin. Although the hypoglycaemia is often life-threatening and initiation of targeted therapies critical, the diagnosis is often delayed and attributable to various factors including: the fact that existence of the condition is not universally accepted; the need to exclude surreptitious causes of hypoglycaemia; the diverse and often complex nature of the glycaemic dysregulation; and the challenge of diagnostic confirmation. Once confirmed, the available therapeutic options are expansive and the reported responses to these therapies have been variable. This review will focus on our evolving understanding, and the associated diagnostic challenges - both clinical and laboratory - of this complex condition.
Conflict of interest statement
Competing Interests: None declared.
Figures
References
-
- Ismail AA. The insulin autoimmune syndrome (IAS) as a cause of hypoglycaemia: an update on the pathophysiology, biochemical investigations and diagnosis. Clin Chem Lab Med. 2016;54:1715–24. - PubMed
-
- Hirata Y, Ishizu H, Ouchi N, Motomura S, Abe Y, Hara M, et al. Insulin autoimmunity in a case of spontaneous hypoglycemia. J Japan Diabetes Soc. 1970;13:312–20.
-
- Archambeaud-Mouveroux F, Huc MC, Nadalon S, Fournier MP, Canivet B. Autoimmune insulin syndrome. Biomed Pharmacoth. 1989;43:581–6. - PubMed
-
- Klein RF, Seino S, Sanz N, Nolte MS, Vinik AI, Karam JH. High performance liquid chromatography used to distinguish the autoimmune hypoglycemia syndrome from factitious hypoglycemia. J Clin Endocrinol Metab. 1985;61:571–4. - PubMed
Publication types
LinkOut - more resources
Full Text Sources