

Blast in Context: The Neuropsychological and Neurocognitive Effects of Long-Term Occupational Exposure to Repeated Low-Level Explosives on Canadian Armed Forces' Breaching Instructors and Range Staff
- PMID: 33343492
- PMCID: PMC7744759
- DOI: 10.3389/fneur.2020.588531
Blast in Context: The Neuropsychological and Neurocognitive Effects of Long-Term Occupational Exposure to Repeated Low-Level Explosives on Canadian Armed Forces' Breaching Instructors and Range Staff
Abstract
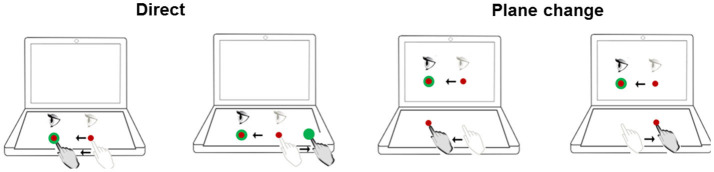
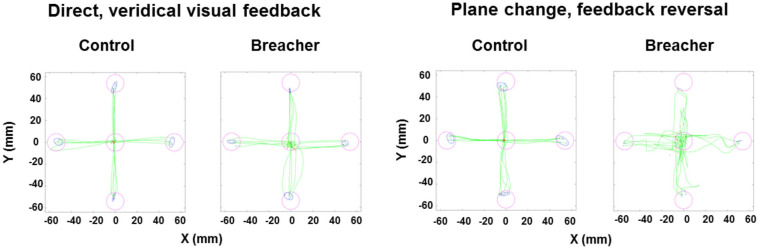
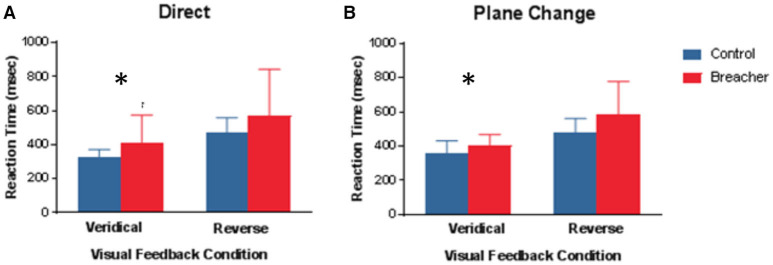
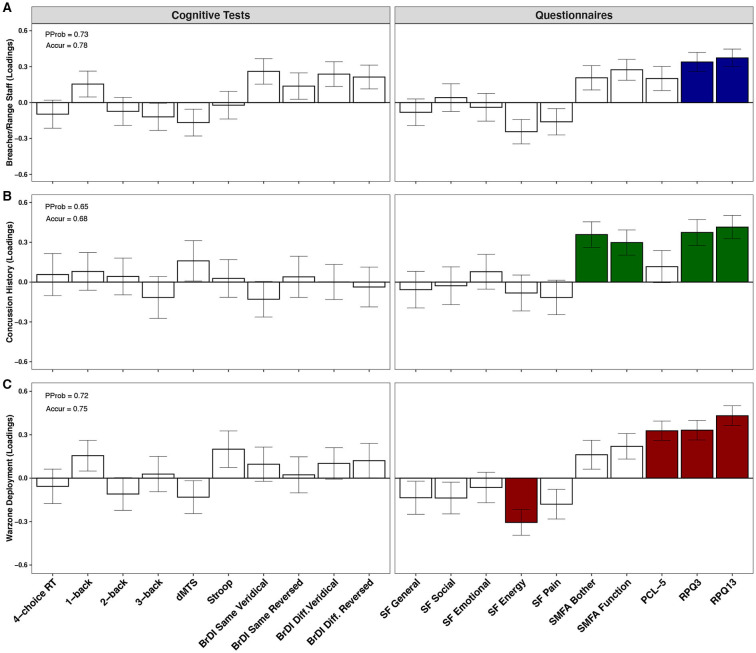
Currently, there is strong interest within the military to better understand the effects of long-term occupational exposure to repeated low-level blast on health and performance. To gain traction on the chronic sequelae of blast, we focused on breaching-a tactical technique for gaining entry into closed/blocked spaces by placing explosives and maintaining a calculated safe distance from the detonation. Using a cross-sectional design, we compared the neuropsychological and neurocognitive profiles of breaching instructors and range staff to sex- and age-matched Canadian Armed Forces (CAF) controls. Univariate tests demonstrated that breaching was associated with greater post-concussive symptoms (Rivermead Post Concussion Symptoms Questionnaire) and lower levels of energy (RAND SF-36). In addition, breaching instructors and range staff were slower on a test that requires moving and thinking simultaneously (i.e., cognitive-motor integration). Next, using a multivariate approach, we explored the impact of other possible sources of injury, including concussion and prior war-zone deployment on the same outcomes. Concussion history was associated with higher post-concussive scores and musculoskeletal problems, whereas deployment was associated with higher post-concussive scores, but lower energy and greater PTSD symptomatology (using PCL-5). Our results indicate that although breaching, concussion, and deployment were similarly correlated with greater post-concussive symptoms, concussion history appears to be uniquely associated with altered musculoskeletal function, whereas deployment history appears to be uniquely associated with lower energy and risk of PTSD. We argue that the broader injury context must, therefore, be considered when studying the impact of repetitive low-level explosives on health and performance in military members.
Keywords: TBI; blast; cognitive motor integration; concussion; military personnel.
Copyright © 2020 Her Majesty the Queen in Right of Canada.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
-
- Greer N, Sayer N, Kramer M, Koeller E, Velasquez T, Wilt TJ. Prevalence and Epidemiology of Combat Blast Injuries From the Military Cohort 2001-2014. VA ESP Project #09-009. Washington, DC: Department of Veterans Affairs; (2016). - PubMed
LinkOut - more resources
Full Text Sources
Research Materials