

Optimizing Patient Selection for Interhospital Transfer and Endovascular Therapy in Acute Ischemic Stroke: Real-World Data From a Supraregional, Hub-and-Spoke Neurovascular Network in Germany
- PMID: 33343500
- PMCID: PMC7746873
- DOI: 10.3389/fneur.2020.600917
Optimizing Patient Selection for Interhospital Transfer and Endovascular Therapy in Acute Ischemic Stroke: Real-World Data From a Supraregional, Hub-and-Spoke Neurovascular Network in Germany
Abstract
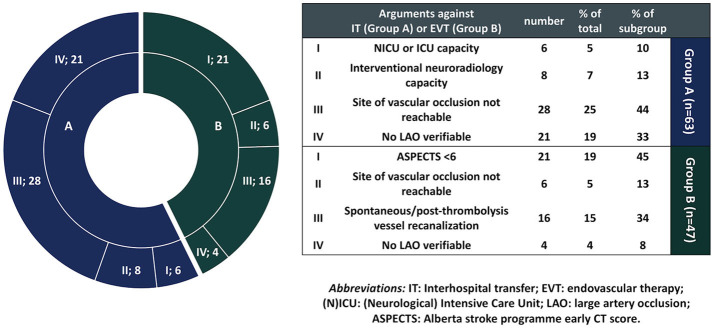
Background: Interhospital transfer for endovascular treatment (EVT) within neurovascular networks might result in transfer of patients who will not undergo EVT (futile transfer). Limited evidence exists on factors associated with the primary patient selection for interhospital transfer from primary stroke centers (PSCs) to comprehensive stroke centers (CSCs), or EVT-workflow parameters that may render a transfer futile. Methods: A prospective, registry-based study was performed between July 1, 2017 and June 30, 2018, at a hub-and-spoke neurovascular network in southwest Germany, comprising 12 referring PSCs and one designated CSC providing round-the-clock EVT at the University Hospital Tübingen. Patients with acute ischemic stroke due to suspected large artery occlusion (LAO) were included upon emergency interhospital transfer inquiry (ITI). Results: ITI was made for 154 patients, 91 (59%) of whom were transferred to the CSC. Non-transferred patients (41%) had significantly higher premorbid modified Rankin scale scores (mRS) compared to transferred patients [median (IQR): 2 (1-3) vs. 0 (0-1), p < 0.001]. Interhospital transfer was denied due to: distal vessel occlusion (44.4%), or non-verifiable LAO (33.3%) in computed tomography angiography (CTA) upon teleconsultation by CSC neuroradiologists; limited Stroke-Unit or ventilation capacity (9.5%), or limited neuroradiological capacity at the CSC (12.7%). The CT-to-ITI interval was significantly longer in patients denied interhospital transfer [median (IQR): 43 (29-56) min] compared to transferred patients [29 (15-55), p = 0.029]. No further differences in EVT-workflow, and no differences in the 3-month mRS outcomes were noted between non-transferred and transferred patients [median (IQR): 2 (0-5) vs. 3 (1-4), p = 0.189]. After transfer to the CSC, 44 (48%) patients underwent EVT. The Alberta stroke program early CT score [ORadj (95% CI): 1.786 (1.573-2.028), p < 0.001] and the CT-to-ITI interval [0.994 (0.991-0.998), p = 0.001] were significant predictors of the likelihood of EVT performance. Conclusion: Our findings show that hub-and-spoke neurovascular network infrastructures efficiently enable access to EVT to patients with AIS due to LAO, who are primarily admitted to PSCs without on-site EVT availability. As in real-world settings optimal allocation of EVT resources is warranted, teleconsultation by experienced endovascular interventionists and prompt interhospital-transfer-inquiries are crucial to reduce the futile transfer rates and optimize patient selection for EVT within neurovascular networks.
Keywords: acute ischemic stroke; endovascular therapy; mechanical thrombectomy; neurovascular network; recanalization.
Copyright © 2020 Stefanou, Stadler, Baku, Hennersdorf, Ernemann, Ziemann, Poli and Mengel.
Conflict of interest statement
SP received speaker's honoraria and consulting honoraria from Bayer, Boehringer-Ingelheim, Bristol-Myers Squibb/Pfizer, Daiichi Sankyo and Werfen, reimbursement for congress traveling and accommodation from Bayer and Boehringer-Ingelheim, and research support from Bristol-Myers Squibb/Pfizer (significant), Boehringer-Ingelheim, Daiichi Sankyo (significant), and Helena Laboratories (all other contributions: modest). All competing interest are outside of the present work. UZ has received grants from European Research Council, German Research Foundation, German Ministry of Education and Research, Biogen Idec GmbH, Servier, and Janssen Pharmaceuticals NV, all not related to this work; and consulting honoraria from Biogen Idec GmbH, Bayer Vital GmbH, Bristol Myers Squibb GmbH, Pfizer, CorTec GmbH, Medtronic GmbH, all not related to this work. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Sacks D, Baxter B, Campbell BCV, Carpenter JS, Cognard C, Dippel D, et al. Multisociety consensus quality improvement revised consensus statement for endovascular therapy of acute ischemic stroke: from the American Association of Neurological Surgeons (AANS), American Society of Neuroradiology (ASNR), Cardiovascular and Interventional Radiology Society of Europe (CIRSE), Canadian Interventional Radiology Association (CIRA), Congress of Neurological Surgeons (CNS), European Society of Minimally Invasive Neurological Therapy (ESMINT), European Society of Neuroradiology (ESNR), European Stroke Organization (ESO), Society for Cardiovascular Angiography and Interventions (SCAI), Society of Interventional Radiology (SIR), Society of NeuroInterventional Surgery (SNIS), and World Stroke Organization (WSO). J Vasc Interv Radiol. (2018) 29:441–53. 10.1016/j.jvir.2017.11.026 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials