

Innate lymphoid cell composition associates with COVID-19 disease severity
- PMID: 33343897
- PMCID: PMC7734472
- DOI: 10.1002/cti2.1224
Innate lymphoid cell composition associates with COVID-19 disease severity
Abstract
Objectives: The role of innate lymphoid cells (ILCs) in coronavirus disease 2019 (COVID-19), caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), is unknown. Understanding the immune response in COVID-19 could contribute to unravel the pathogenesis and identification of treatment targets. Here, we describe the phenotypic landscape of circulating ILCs in COVID-19 patients and identified ILC phenotypes correlated to serum biomarkers, clinical markers and laboratory parameters relevant in COVID-19.
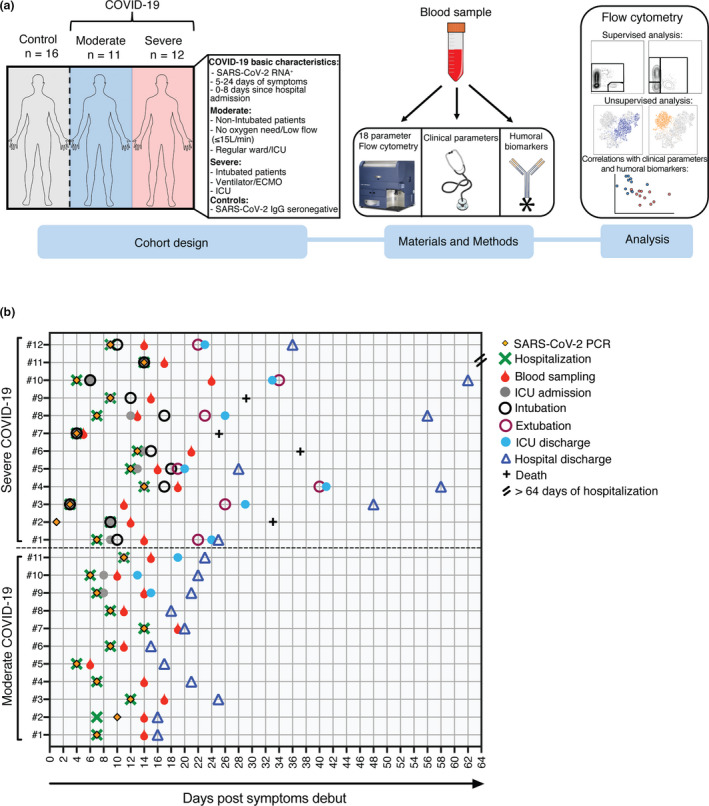
Methods: Blood samples collected from moderately (n = 11) and severely ill (n = 12) COVID-19 patients, as well as healthy control donors (n = 16), were analysed with 18-parameter flow cytometry. Using supervised and unsupervised approaches, we examined the ILC activation status and homing profile. Clinical and laboratory parameters were obtained from all COVID-19 patients, and serum biomarkers were analysed with multiplex immunoassays.
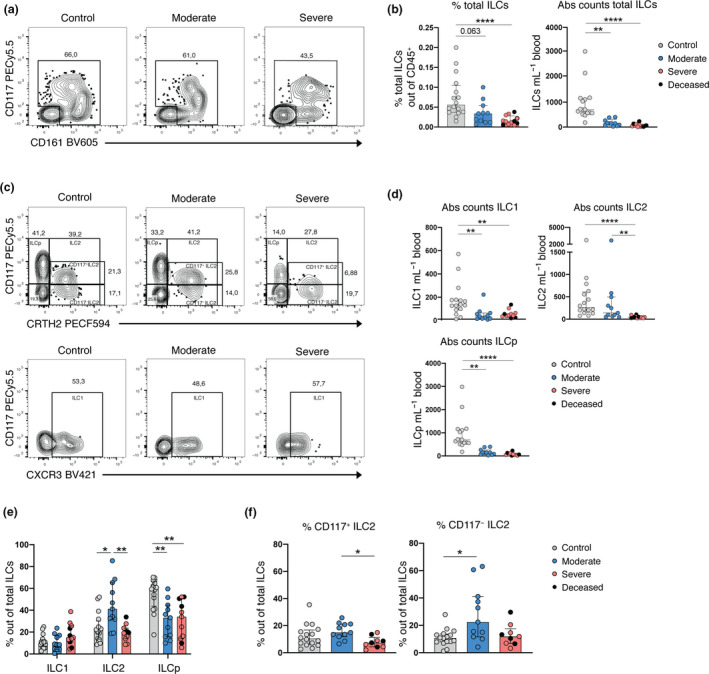
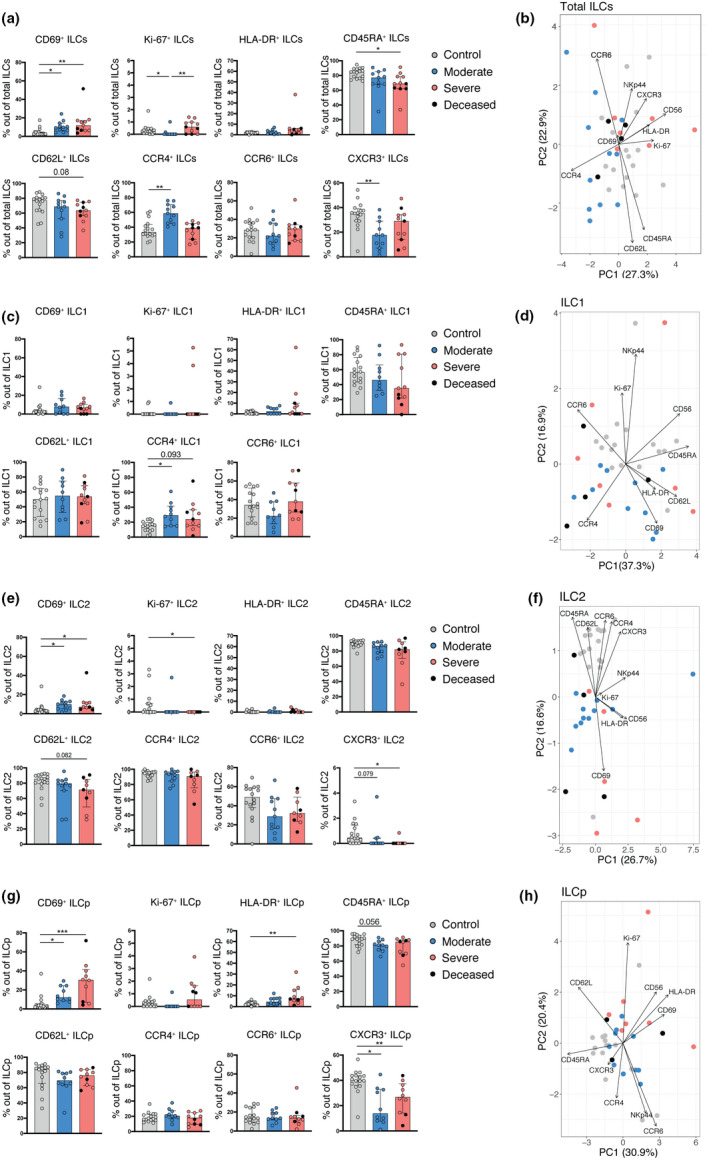
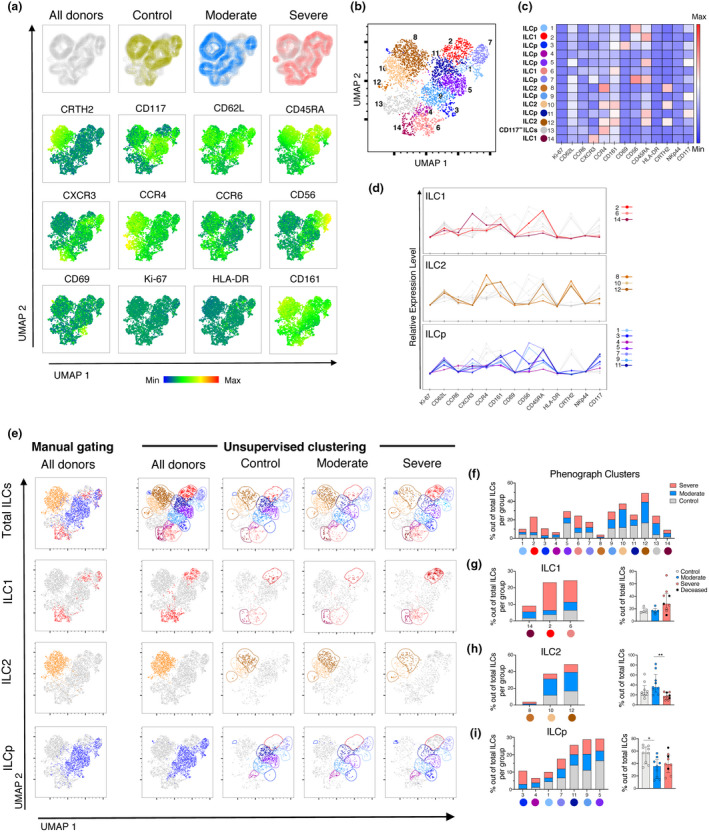
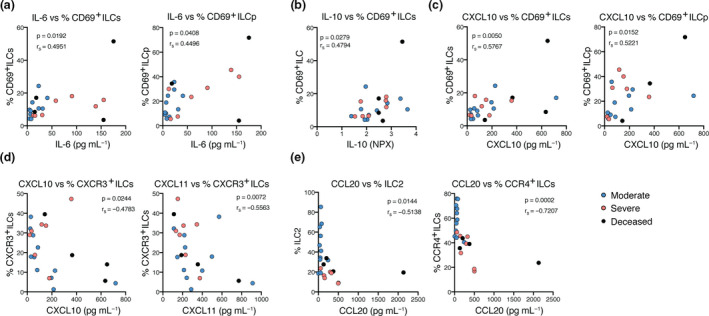
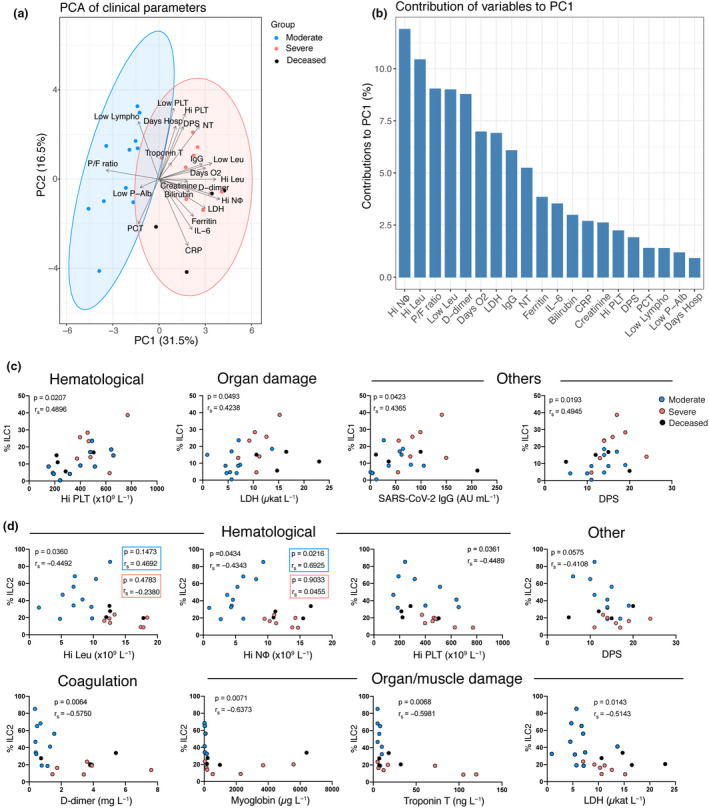
Results: Innate lymphoid cells were largely depleted from the circulation of COVID-19 patients compared with healthy controls. Remaining circulating ILCs revealed decreased frequencies of ILC2 in severe COVID-19, with a concomitant decrease of ILC precursors (ILCp) in all patients, compared with controls. ILC2 and ILCp showed an activated phenotype with increased CD69 expression, whereas expression levels of the chemokine receptors CXCR3 and CCR4 were significantly altered in ILC2 and ILCp, and ILC1, respectively. The activated ILC profile of COVID-19 patients was associated with soluble inflammatory markers, while frequencies of ILC subsets were correlated with laboratory parameters that reflect the disease severity.
Conclusion: This study provides insights into the potential role of ILCs in immune responses against SARS-CoV-2, particularly linked to the severity of COVID-19.
Keywords: COVID‐19; SARS‐CoV‐2; coronavirus; immune response; innate lymphoid cells; respiratory viral infection.
© 2020 The Authors. Clinical & Translational Immunology published by John Wiley & Sons Australia, Ltd on behalf of Australian and New Zealand Society for Immunology, Inc.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. HGL is a member of the board of XNK Therapeutics AB and Vycellix Inc.
Figures
References
-
- Le Thanh T, Andreadakis Z, Kumar A et al The COVID‐19 vaccine development landscape. Nat Rev Drug Discov 2020; 19: 305–306. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous