

Hemorrhagic corpus luteum: Clinical management update
- PMID: 33343977
- PMCID: PMC7731611
- DOI: 10.4274/tjod.galenos.2020.40359
Hemorrhagic corpus luteum: Clinical management update
Abstract
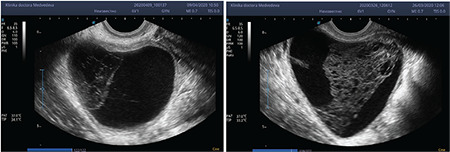
Hemorrhagic corpus luteum (HCL) is an ovarian cyst formed after ovulation and caused by spontaneous bleeding into a corpus luteum (CL) cyst. When HCL rupture happens, a hemoperitoneum results. Clinical symptoms are mainly due to peritoneal irritation by the blood effusion. The differential diagnosis is extensive and standard management is not defined. The authors elaborated a comparison of the differential diagnosis and therapeutic modalities from the laparoscopic approach to nonsurgical, medical options because hemorrhage from HCL is often self-limiting. The authors reviewed all data implicated with the development of HCL, trying to give homogeneity to literature data. The authors analyzed extensive literature data and subdivided the medical approach into many topics. The wait-and-see attitude avoids unnecessary laparoscopic surgery using supportive therapies (antifibrinolytic, analgesics, liquid infusion, transfusions and antibiotic prophylaxis). Surgical therapy: operative management should be laparoscopic, with surgical options such as luteumectomy, ovarian wedge-shaped excision or oophorectomy. Prevention: the possibility to preserve fertility is essential, mainly in patients with bleeding disorders or undergoing anticoagulant therapy; therefore, they need estro-progestinics or GnRH analogues to prevent ovulation and avoid further episodes of HCL. This review will aid physicians in making an early diagnosis of HCL, to avoid unnecessary surgery, and use the most effective treatment.
Keywords: Corpus luteum; ectopic pregnancy; laparoscopy; ovarian cyst.
©Copyright 2020 by Turkish Society of Obstetrics and Gynecology | Turkish Journal of Obstetrics and Gynecology published by Galenos Publishing House.
Conflict of interest statement
Conflict of Interest: No conflict of interest was declared by the authors.
Figures


Similar articles
-
Corpus luteum hemorrhage with acquired hemophilia A: a case report and literature review.BMC Womens Health. 2022 Oct 11;22(1):418. doi: 10.1186/s12905-022-02000-9. BMC Womens Health. 2022. PMID: 36221134 Free PMC article. Review.
-
Management of ruptured corpus luteum cyst of pregnancy occurring in a 15-year-old girl by laparoscopic surgery with intraoperative autologous blood transfusion.J Pediatr Adolesc Gynecol. 2007 Apr;20(2):97-100. doi: 10.1016/j.jpag.2006.09.017. J Pediatr Adolesc Gynecol. 2007. PMID: 17418394
-
MANAGEMENT OF RUPTURED CORPUS LUTEUM WITH HEMOPERITONEUM IN EARLY PREGNANCY - A CASE REPORT.Acta Clin Croat. 2018 Dec;57(4):785-788. doi: 10.20471/acc.2018.57.04.24. Acta Clin Croat. 2018. PMID: 31168219 Free PMC article.
-
Ruptured corpus luteum with hemoperitoneum: a study of 173 surgical cases.Am J Obstet Gynecol. 1984 May 1;149(1):5-9. doi: 10.1016/0002-9378(84)90282-5. Am J Obstet Gynecol. 1984. PMID: 6720774
-
Various sonographic appearances of the hemorrhagic corpus luteum cyst.Ultrasound Q. 2004 Jun;20(2):45-58. doi: 10.1097/00013644-200406000-00003. Ultrasound Q. 2004. PMID: 15480190 Review.
Cited by
-
Terminological discrepancies and novelties in the histological description of the female genital system: proposed amendments for clinical-translational anatomy.Anat Sci Int. 2024 Sep;99(4):469-480. doi: 10.1007/s12565-024-00772-8. Epub 2024 Apr 29. Anat Sci Int. 2024. PMID: 38683308 Free PMC article.
-
Heat Stress and Its Impact on Corpus Luteum (CL) Function and Reproductive Efficiency in Mammals: A Critical Review.Reprod Sci. 2025 Apr;32(4):977-992. doi: 10.1007/s43032-025-01787-w. Epub 2025 Feb 3. Reprod Sci. 2025. PMID: 39900848
-
Corpus luteum hemorrhage with acquired hemophilia A: a case report and literature review.BMC Womens Health. 2022 Oct 11;22(1):418. doi: 10.1186/s12905-022-02000-9. BMC Womens Health. 2022. PMID: 36221134 Free PMC article. Review.
-
Laparoscopic surgery for left ovarian hemorrhage in a patient with an implantable left ventricular assist device on antithrombotic therapy and a history of right salpingo-oophorectomy open surgery for right ovarian bleeding: A case report.Case Rep Womens Health. 2024 Nov 23;44:e00669. doi: 10.1016/j.crwh.2024.e00669. eCollection 2024 Dec. Case Rep Womens Health. 2024. PMID: 39687743 Free PMC article.
-
Ruptured Corpus Luteum among Women Undergoing Laparotomy for Hemoperitoneum in a Tertiary Care Centre: A Descriptive Cross-sectional Study.JNMA J Nepal Med Assoc. 2023 Feb 1;61(258):137-140. doi: 10.31729/jnma.7987. JNMA J Nepal Med Assoc. 2023. PMID: 37203987 Free PMC article.
References
-
- Hallatt JG, Steele CH Jr, Snyder M. Ruptured corpus luteum with hemoperitoneum: a study of 173 surgical cases. Am J Obset Gynecol. 1984;149:5–9. - PubMed
-
- Gupta N, Dadhwal V, Deka D, Jain SK, Mittal S. Corpus luteum hemorrhage: rare complication of congenital and acquired coagulation abnormalities. J Obstet Gynaecol. 2007;33:376–80. - PubMed
-
- Aggarwal A, Goel P, Wanchu M, Malhotra R, Malhotra S. Ruptured corpus luteum with hemoperitoneum. J Obstet Gynecol Ind. 2004;54:488–90.
-
- Novak ER, Woodruff JD. Gynecologic and Obstetric Pathology. 7th edition. vol. 17. Philadelphia: WB Saunders Co. 1974;.p.:334–40.
-
- Tang LC, Cho HK, Chan SY, Wong VC. Dextropreponderance of corpus luteum rupture: a clinical study. J Reprod Med. 1985;30:764–8. - PubMed
Publication types
LinkOut - more resources
Full Text Sources