

Outcomes of COVID-19 Among Hospitalized Patients With Non-dialysis CKD
- PMID: 33344488
- PMCID: PMC7744802
- DOI: 10.3389/fmed.2020.615312
Outcomes of COVID-19 Among Hospitalized Patients With Non-dialysis CKD
Abstract
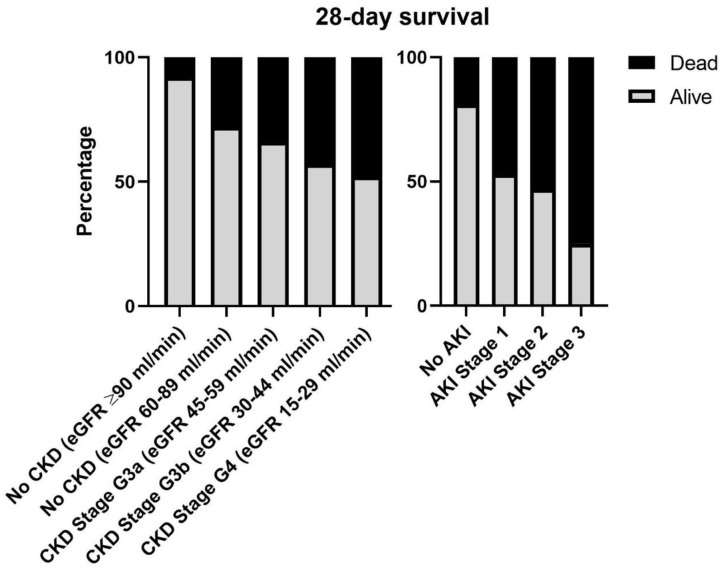
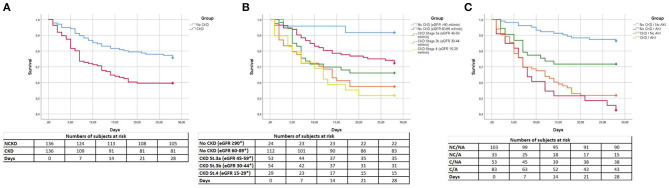
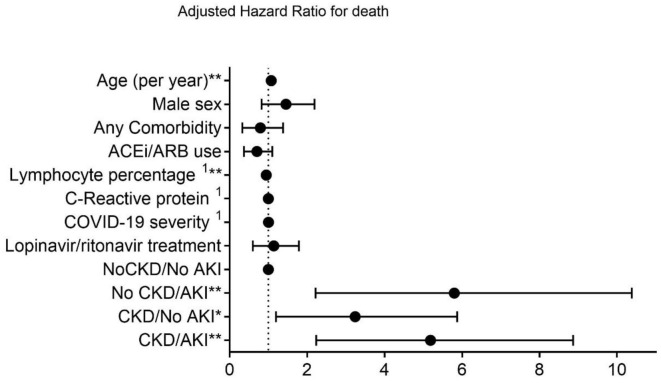
Background: Coronavirus disease 2019 (COVID-19), caused by Severe Acute Respiratory Syndrome-Corona Virus 2 has generated significant impact on global health worldwide. COVID-19 can cause pneumonia and organ injury. Chronic kidney disease (CKD) has been associated with increased mortality in previous epidemics, but there is a paucity of data regarding actual risks for non-dialysis CKD patients with COVID-19. Methods: Multicenter, observational cohort study including 136 non-dialysis CKD patients and 136 age- and sex-matched controls that required hospitalization due to COVID-19. Patients with end-stage renal disease, a kidney transplant or without registered baseline glomerular filtration rate prior to COVID-19 infection were excluded. CKD and acute kidney injury (AKI) were defined according to KDIGO criteria. Results: CKD patients had higher white blood cell count and D-dimer and lower lymphocyte percentage. No differences were found regarding symptoms on admission. CKD was associated with higher rate of AKI (61 vs. 24.3%) and mortality (40.4 vs. 24.3%). Patients with AKI had the highest hazard for death (AKI/non-CKD HR:7.04, 95% CI:2.87-17.29; AKI/CKD HR:5.25, 95% CI: 2.29-12.02), followed by CKD subjects without AKI (HR:3.39, 95% CI:1.36-8.46). CKD status did not condition ICU admission or length of in-hospital stay. Conclusions: CKD patients that require hospitalization due to COVID-19 are exposed to higher risk of death and AKI.
Keywords: COVID−19; acute kidney damage; chornic kidney disease; pneumonia; renal failure.
Copyright © 2020 Coca, Burballa, Centellas-Pérez, Pérez-Sáez, Bustamante-Munguira, Ortega, Dueñas, Arenas, Pérez-Martínez, Ruiz, Crespo, Llamas, Bustamante-Munguira and Pascual.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
LinkOut - more resources
Full Text Sources