

Nonhypertensive male with multiple paragangliomas of the heart and neck: A case report
- PMID: 33344564
- PMCID: PMC7716317
- DOI: 10.12998/wjcc.v8.i22.5707
Nonhypertensive male with multiple paragangliomas of the heart and neck: A case report
Abstract
Background: Paraganglioma is a rare disease that can be lethal if undiagnosed. Thus, quick recognition is very important. Cardiac paragangliomas are found in patients who have hypertension. The classic symptoms are the triad of headaches, palpitations, and profuse sweating. We describe a very rare case of multiple paragangliomas of the heart and bilateral carotid artery without hypertension and outline the management strategies for this disease.
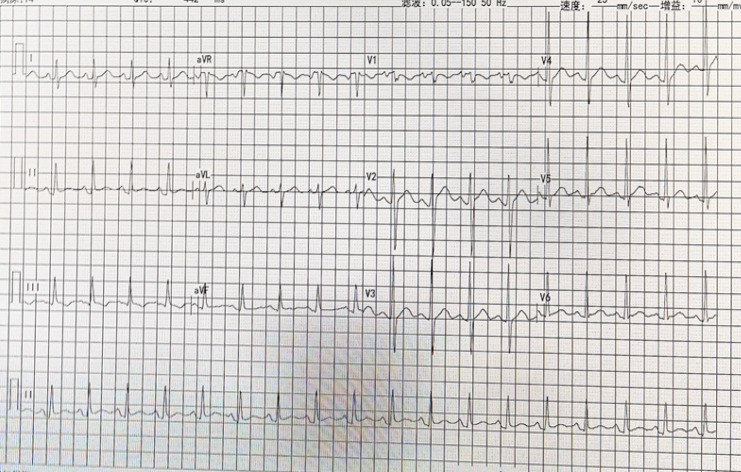
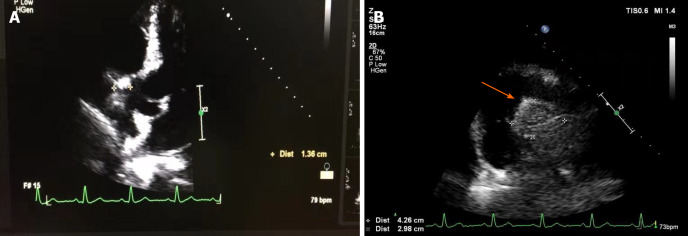
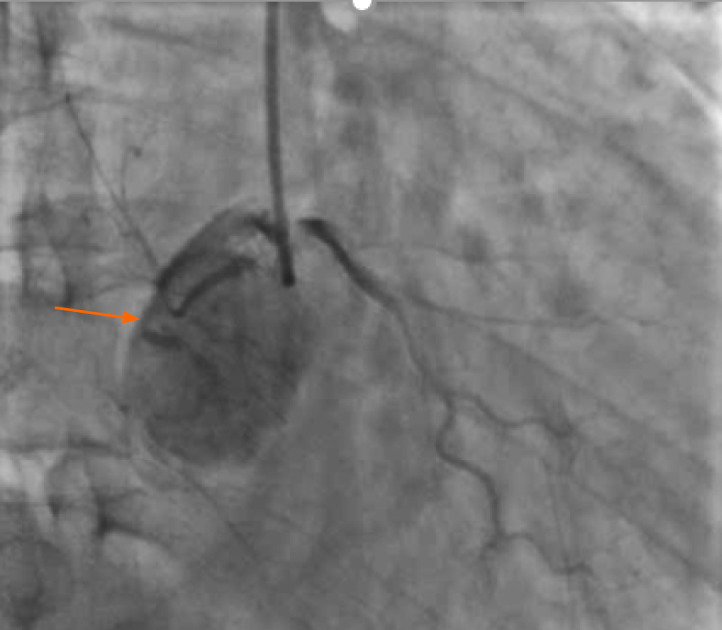
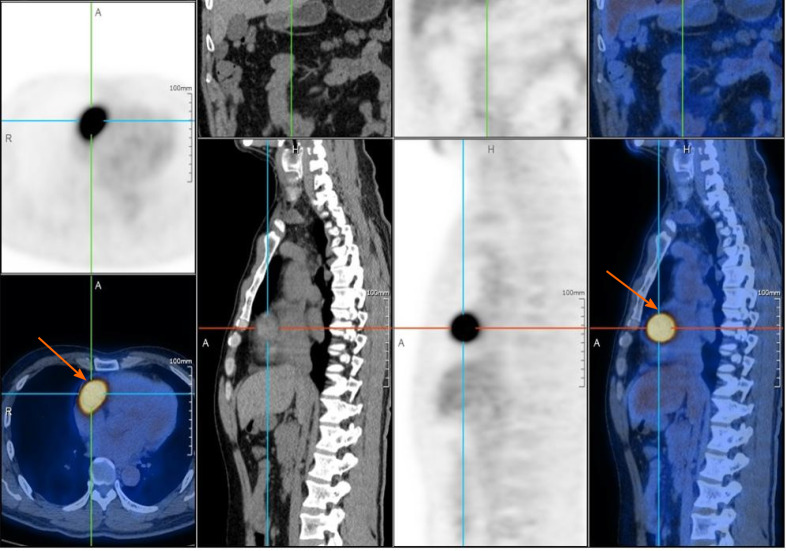
Case summary: A 46-year-old man presented with the chief complaint of recently recurrent chest pain with a history of hemangioma of the bilateral carotid artery that had been surgically removed. He was found to have an intracardiac mass in the right atrioventricular groove and underwent successful excision. The final pathology demonstrated that the intracardiac mass was a cardiac paraganglioma, and the patient had an increased level of normetanephrine in the blood. The pathology and immunohistochemistry results showed that the bilateral carotid masses were also paragangliomas. During the 3 mo follow-up period, the patient did not experience recurrence of chest pain.
Conclusion: To our knowledge, this is the first case of multiple paragangliomas of the heart and neck without hypertension. This rare disease can be lethal if left undiagnosed. Thus, quick recognition is very important. The key to the diagnosis of cardiac paraganglioma is the presence of typical symptoms, including headaches, palpitations, profuse sweating, hypertension, and chest pain. Radiology can demonstrate the intracardiac mass. It is important to determine the levels of normetanephrine in the blood. The detection of genetic mutations is also recommended. Surgical resection is necessary to treat the disease and obtain pathological evidence.
Keywords: Cardiac paraganglioma; Case report; Chest pain; Intracardiac mass; Normetanephrine; Pathological evidence.
©The Author(s) 2020. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors declare that they have no conflicts of interest.
Figures

References
-
- Neumann HPH, Young WF Jr, Eng C. Pheochromocytoma and Paraganglioma. N Engl J Med. 2019;381:552–565. - PubMed
-
- Berends AMA, Buitenwerf E, de Krijger RR, Veeger NJGM, van der Horst-Schrivers ANA, Links TP, Kerstens MN. Incidence of pheochromocytoma and sympathetic paraganglioma in the Netherlands: A nationwide study and systematic review. Eur J Intern Med. 2018;51:68–73. - PubMed
-
- Karabinos I, Rouska E, Charokopos N. A primary cardiac paraganglioma. Eur Heart J. 2012;33:790. - PubMed
-
- Neumann HP. Pheochromocytoma. In: Jameson JL, Fauci AS, Kasper DL, Hauser SL, Longo DL, Loscalzo J. Harrison’s principles of internal medicine. 20th ed. New York: McGraw Hill Education; 2018: 2739-2746.
-
- Lloyd RV, Osamura RY, Klöppel G, Rosai J. Phaechromocytoma. In: WHO classification of tumours of endocrine organs. 4th ed. Lyon, France: International Agency for Research on Cancer; 2017: 183-190.
Publication types
LinkOut - more resources
Full Text Sources
