

Neuronal intranuclear inclusion disease mimicking acute cerebellitis: A case report
- PMID: 33344613
- PMCID: PMC7723690
- DOI: 10.12998/wjcc.v8.i23.6122
Neuronal intranuclear inclusion disease mimicking acute cerebellitis: A case report
Abstract
Background: Neuronal intranuclear inclusion disease (NIID) is an unusual autosomal dominant, chronic progressive neurodegenerative disease. The clinical manifestations of NIID are complex and varied, complicating its clinical diagnosis. To the best of our knowledge, this report is the first to document sporadic adult-onset NIID mimicking acute cerebellitis (AC) that was finally diagnosed by imaging studies, skin biopsy, and genetic testing.
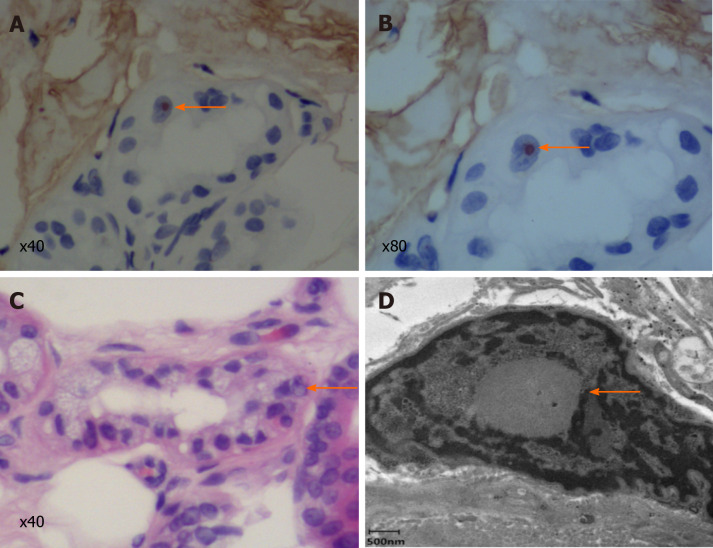
Case summary: A 63-year-old man presented with fever, gait unsteadiness, dysarthria, and an episode of convulsion. His serum levels of white blood cells and C-reactive protein were significantly elevated. T2-weighted brain magnetic resonance imaging and fluid attenuation inversion recovery sequences showed bilateral high-intensity signals in the medial part of the cerebellar hemisphere beside the vermis. While we initially considered a diagnosis of AC, the patient's symptoms improved significantly without special treatment, prompting our consideration of NIID. Diffusion-weighted imaging showed hyperintensity in the corticomedullary junction. Skin biopsy revealed eosinophilic inclusions positive for anti-p62 in epithelial sweat-gland cells. GGC repeat expansions in the Notch 2 N-terminal like C gene confirmed the diagnosis of NIID.
Conclusion: For patients with clinical manifestations mimicking AC, the possibility of underlying NIID should be considered along with prompt rigorous examinations.
Keywords: Acute cerebellitis; Case report; Genetic testing; Magnetic resonance imaging; Neuronal intranuclear inclusion disease; Skin biopsy.
©The Author(s) 2020. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors declare that they have no conflict of interest to report.
Figures



References
-
- Deng J, Gu M, Miao Y, Yao S, Zhu M, Fang P, Yu X, Li P, Su Y, Huang J, Zhang J, Yu J, Li F, Bai J, Sun W, Huang Y, Yuan Y, Hong D, Wang Z. Long-read sequencing identified repeat expansions in the 5'UTR of the NOTCH2NLCgene from Chinese patients with neuronal intranuclear inclusion disease. J Med Genet. 2019;56:758–764. - PubMed
-
- Takahashi-Fujigasaki J. Neuronal intranuclear hyaline inclusion disease. Neuropathology. 2003;23:351–359. - PubMed
-
- Sone J, Mori K, Inagaki T, Katsumata R, Takagi S, Yokoi S, Araki K, Kato T, Nakamura T, Koike H, Takashima H, Hashiguchi A, Kohno Y, Kurashige T, Kuriyama M, Takiyama Y, Tsuchiya M, Kitagawa N, Kawamoto M, Yoshimura H, Suto Y, Nakayasu H, Uehara N, Sugiyama H, Takahashi M, Kokubun N, Konno T, Katsuno M, Tanaka F, Iwasaki Y, Yoshida M, Sobue G. Clinicopathological features of adult-onset neuronal intranuclear inclusion disease. Brain. 2016;139:3170–3186. - PMC - PubMed
-
- Sone J, Mitsuhashi S, Fujita A, Mizuguchi T, Hamanaka K, Mori K, Koike H, Hashiguchi A, Takashima H, Sugiyama H, Kohno Y, Takiyama Y, Maeda K, Doi H, Koyano S, Takeuchi H, Kawamoto M, Kohara N, Ando T, Ieda T, Kita Y, Kokubun N, Tsuboi Y, Katoh K, Kino Y, Katsuno M, Iwasaki Y, Yoshida M, Tanaka F, Suzuki IK, Frith MC, Matsumoto N, Sobue G. Long-read sequencing identifies GGC repeat expansions in NOTCH2NLC associated with neuronal intranuclear inclusion disease. Nat Genet. 2019;51:1215–1221. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
