

Endobronchial Valves for the Treatment of Advanced Emphysema
- PMID: 33345947
- PMCID: PMC8129734
- DOI: 10.1016/j.chest.2020.12.007
Endobronchial Valves for the Treatment of Advanced Emphysema
Abstract
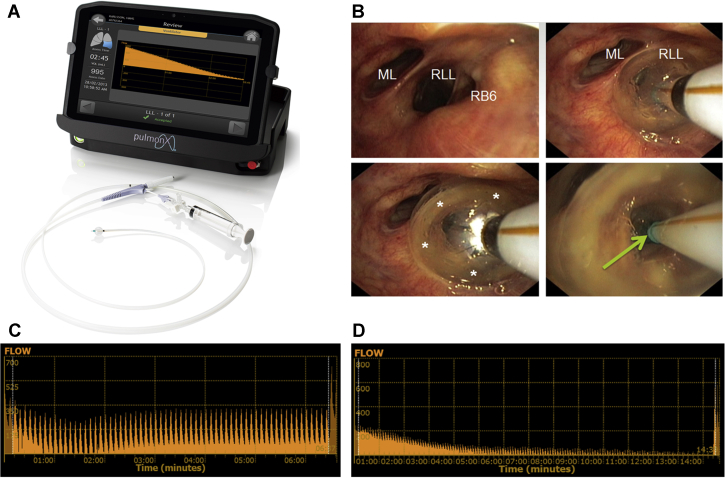
Bronchoscopic lung volume reduction with one-way endobronchial valves is a guideline treatment option for patients with advanced emphysema that is supported by extensive scientific data. Patients limited by severe hyperinflation, with a suitable emphysema treatment target lobe and with absence of collateral ventilation, are the responders to this treatment. Detailed patient selection, a professional treatment performance, and dedicated follow up of the valve treatment, including management of complications, are key ingredients to success. This treatment does not stand alone; it especially requires extensive knowledge of COPD for which the most appropriate treatment is discussed in a multidisciplinary approach. We discuss the endobronchial valve treatment for emphysema and provide a guideline for patient selection, treatment guidance, and practice tools, based on our own experience and literature.
Keywords: COPD; bronchoscopy; emphysema; endobronchial valve; lung volume reduction.
Copyright © 2020 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Klooster K., ten Hacken N.H., Hartman J.E., Kerstjens H.A., van Rikxoort E.M., Slebos D.J. Endobronchial valves for emphysema without interlobar collateral ventilation. N Engl J Med. 2015;373(24):2325–2335. - PubMed
-
- Shah P.L., Slebos D.J. Bronchoscopic interventions for severe emphysema: where are we now? Respirology. 2020;25(9):972–980. - PubMed
-
- Welling J.B.A., Klooster K., Hartman J.E. Collateral ventilation measurement using chartis: procedural sedation vs general anesthesia. Chest. 2019;156(5):984–990. - PubMed
-
- Criner G.J., Sue R., Wright S. A multicenter randomized controlled trial of zephyr endobronchial valve treatment in heterogeneous emphysema (LIBERATE) Am J Respir Crit Care Med. 2018;198(9):1151–1164. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
