

The Use of Slow Codes and Medically Futile Codes in Practice
- PMID: 33346066
- PMCID: PMC8729118
- DOI: 10.1016/j.jpainsymman.2020.12.001
The Use of Slow Codes and Medically Futile Codes in Practice
Abstract
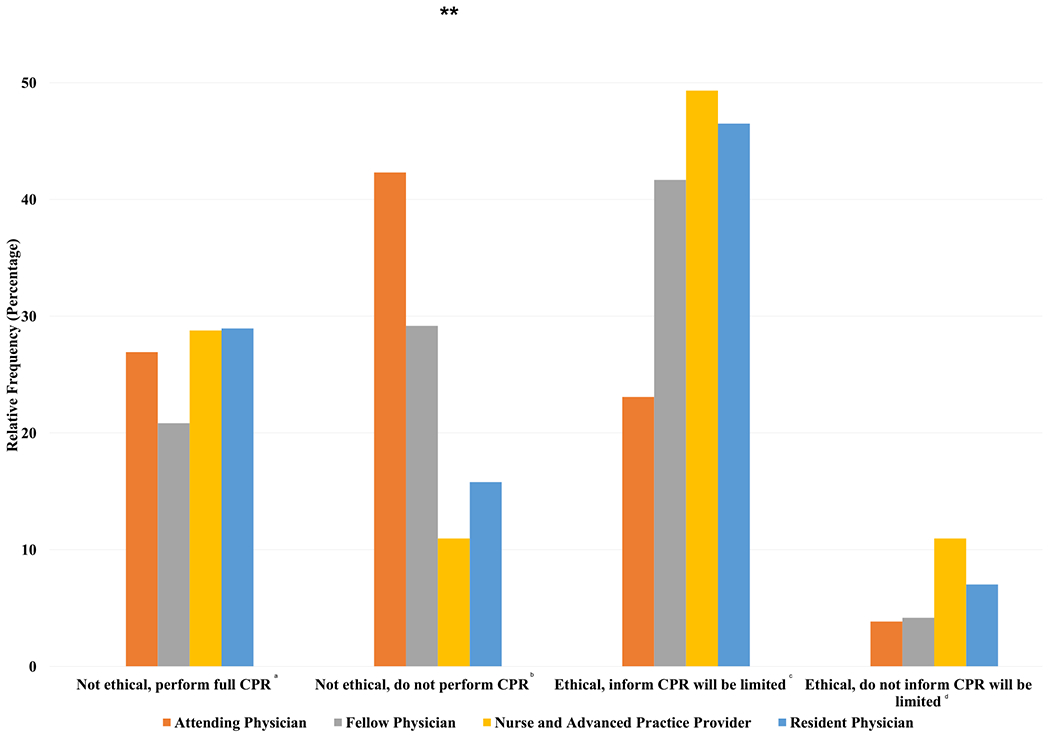
Context: Slow codes, which occur when clinicians symbolically appear to conduct advanced cardiac life support but do not provide full resuscitation efforts, are ethically controversial.
Objectives: To describe the use of slow codes in practice and their association with clinicians' attitudes and moral distress.
Methods: We conducted a cross-sectional survey at Rush University and University of Chicago in January 2020. Participants included physician trainees, attending physicians, nurses, and advanced practice providers who care for critically ill patients.
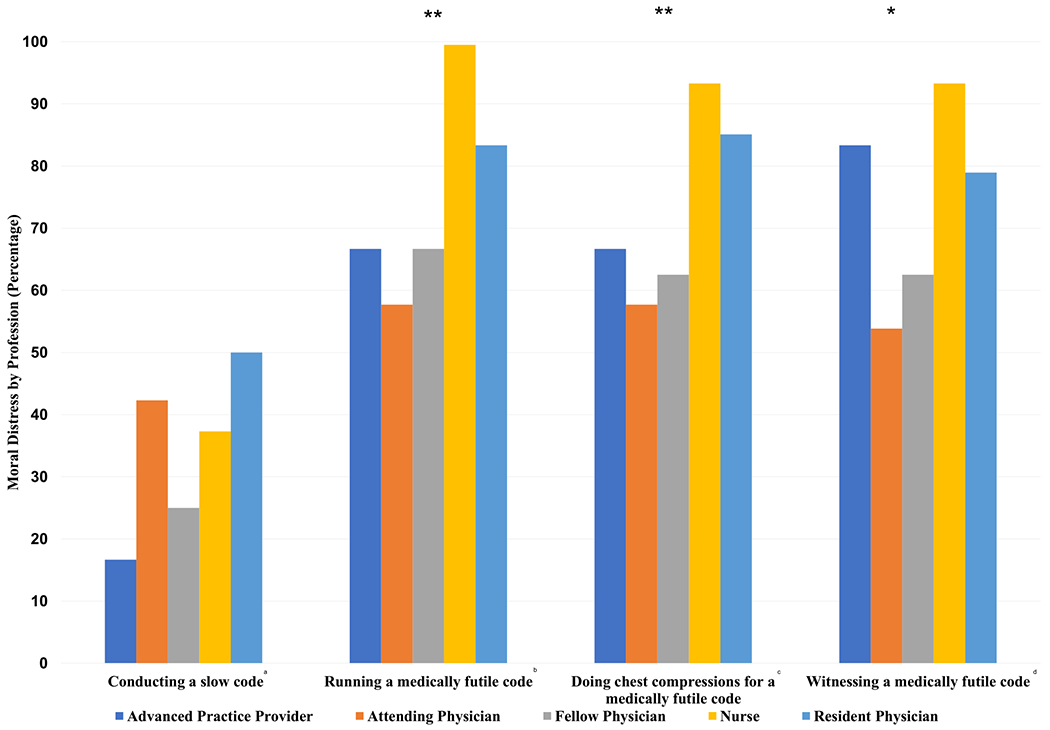
Results: Of the 237 respondents to the survey (31% response rate, n = 237/753), almost half (48%) were internal medicine residents (46% response rate, n = 114/246). Over two-thirds of all respondents (69%) reported caring for a patient where a slow code was performed, with a mean of 1.3 slow codes (SD 1.7) occurring in the past year per participant. A narrow majority of respondents (52%) reported slow codes are ethical if the code is medically futile. Other respondents (46%) reported slow codes are not ethical, with 19% believing no code should be performed and 28% believing a full guideline consistent code should be performed. Most respondents reported moral distress when being required to run (75%), do chest compressions for (80%), or witness (78%) a cardiac resuscitation attempt they believe to be medically futile.
Conclusion: Slow codes occur in practice, even though many clinicians ethically disagree with their use. The use of cardiac resuscitation attempts in medically futile situations can cause significant moral distress to medical professionals who agree or are forced to participate in them.
Keywords: Slow code; clinical medical ethics; critical care; futility; intensive care unit.
Copyright © 2020 American Academy of Hospice and Palliative Medicine. Published by Elsevier Inc. All rights reserved.
Figures

Similar articles
-
Moral dilemmas and slow codes.Bioethics. 2025 May;39(4):359-367. doi: 10.1111/bioe.13399. Epub 2025 Feb 13. Bioethics. 2025. PMID: 39943884
-
Moral Distress Amongst American Physician Trainees Regarding Futile Treatments at the End of Life: A Qualitative Study.J Gen Intern Med. 2016 Jan;31(1):93-9. doi: 10.1007/s11606-015-3505-1. Epub 2015 Sep 21. J Gen Intern Med. 2016. PMID: 26391029 Free PMC article.
-
Veterinary technicians report in a survey how futile veterinary treatments contribute to their moral distress and impact their professional and personal lives.J Am Vet Med Assoc. 2025 Jan 2;263(4):473-482. doi: 10.2460/javma.24.10.0659. Print 2025 Apr 1. J Am Vet Med Assoc. 2025. PMID: 39746297
-
Understanding the moral distress of nurses witnessing medically futile care.Oncol Nurs Forum. 2006 Sep 1;33(5):922-30. doi: 10.1188/06.ONF.922-930. Oncol Nurs Forum. 2006. PMID: 16955120 Review.
-
Rituals, death and the moral practice of medical futility.Nurs Ethics. 2009 May;16(3):292-302. doi: 10.1177/0969733009102691. Nurs Ethics. 2009. PMID: 19372124 Review.
Cited by
-
Shared Decision-Making on Life-Sustaining Treatment: A Survey of Current Barriers in Practice Among Clinicians Across China.Healthcare (Basel). 2025 Mar 3;13(5):547. doi: 10.3390/healthcare13050547. Healthcare (Basel). 2025. PMID: 40077109 Free PMC article.
-
Addressing Futility: A Practical Approach.Crit Care Explor. 2022 Jul 1;4(7):e0706. doi: 10.1097/CCE.0000000000000706. eCollection 2022 Jul. Crit Care Explor. 2022. PMID: 35815180 Free PMC article. Review.
-
Disparities in Unilateral Do Not Resuscitate Order Use During the COVID-19 Pandemic.Crit Care Med. 2023 Aug 1;51(8):1012-1022. doi: 10.1097/CCM.0000000000005863. Epub 2023 Mar 30. Crit Care Med. 2023. PMID: 36995088 Free PMC article.
-
Ethics, orthodoxies and defensive practice: a cross-sectional survey of nurse's decision-making surrounding CPR in deceased inpatients without Do Not Resuscitate orders.BMC Med Ethics. 2025 May 20;26(1):65. doi: 10.1186/s12910-025-01224-2. BMC Med Ethics. 2025. PMID: 40394513 Free PMC article.
-
Addressing Inadequate Documentation of Unilateral Do-Not-Resuscitate Orders.JAMA. 2025 Mar 4;333(9):755-756. doi: 10.1001/jama.2024.26282. JAMA. 2025. PMID: 39804637 Free PMC article.
References
-
- Neumar RW, Shuster M, Callaway CW, et al. American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2015;132:S315–S367. - PubMed
-
- Jonsen AR, Siegler M, Winslade WJ. Clinical ethics: a practical approach to ethical decisions in clinical medicine. Rush University (RSH) —Chicago, IL: [Internet]. Available from https://i-share-rsh.primo.exlibrisgroup.com. Accessed September 27, 2020.
-
- DePalma JA, Ozanich E, Miller S, Yancich LM. “Slow” code: perspectives of a physician and critical care nurse. Crit Care Nurs Q 1999;22:89–97. - PubMed
-
- Ganz FD, Sharfi R, Kaufman N, Einav S. Perceptions of slow codes by nurses working on internal medicine wards. Nurs Ethics 2019;26:1734–1743. - PubMed
-
- Zucker A Law and ethics. Death Stud 2004;28:181–184. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
