

Birthweight and other perinatal outcomes of singletons conceived after assisted reproduction compared to natural conceived singletons in couples with unexplained subfertility: follow-up of two randomized clinical trials
- PMID: 33347597
- PMCID: PMC7891811
- DOI: 10.1093/humrep/deaa298
Birthweight and other perinatal outcomes of singletons conceived after assisted reproduction compared to natural conceived singletons in couples with unexplained subfertility: follow-up of two randomized clinical trials
Abstract
Study question: Does assisted reproduction, such as ovarian stimulation and/or laboratory procedures, have impact on perinatal outcomes of singleton live births compared to natural conception in couples with unexplained subfertility?
Summary answer: Compared to natural conception, singletons born after intrauterine insemination with ovarian stimulation (IUI-OS) had a lower birthweight, while singletons born after IVF had comparable birthweights, in couples with unexplained subfertility.
What is known already: Singletons conceived by assisted reproduction have different perinatal outcomes such as low birthweight and a higher risk of premature birth than naturally conceived singletons. This might be due to the assisted reproduction, such as laboratory procedures or the ovarian stimulation, or to an intrinsic factor in couples with subfertility.
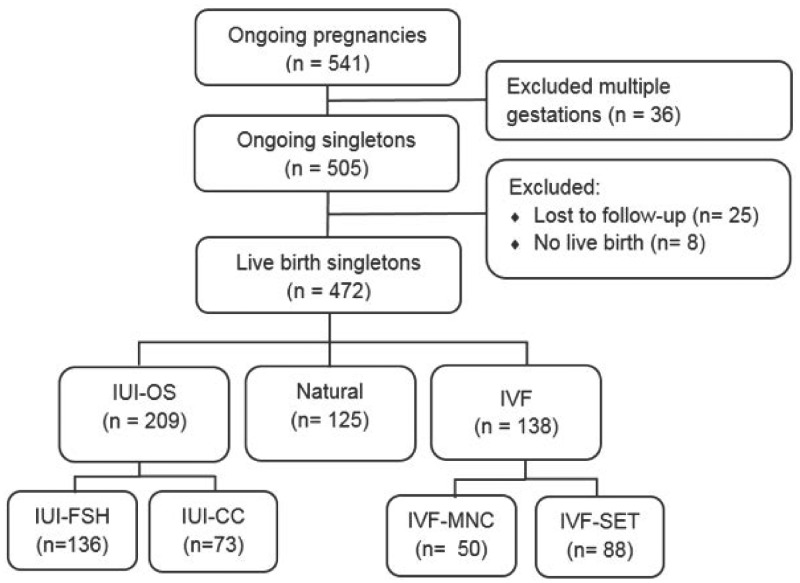
Study design, size, duration: We performed a prospective cohort study using the follow-up data of two randomized clinical trials performed in couples with unexplained subfertility. We evaluated perinatal outcomes of 472 live birth singletons conceived after assisted reproduction or after natural conception within the time horizon of the studies.
Participants/materials, setting, methods: To assess the possible impact of ovarian stimulation we compared the singletons conceived after IUI with FSH or clomiphene citrate (CC) and IVF in a modified natural cycle (IVF-MNC) or standard IVF with single embryo transfer (IVF-SET) to naturally conceived singletons in the same cohorts. To further look into the possible effect of the laboratory procedures, we put both IUI and IVF groups together into IUI-OS and IVF and compared both to singletons born after natural conception. We only included singletons conceived after fresh embryo transfers. The main outcome was birthweight presented as absolute weight in grams and gestational age- and gender-adjusted percentiles. We calculated differences in birthweight using regression analyses adjusted for maternal age, BMI, smoking, parity, duration of subfertility and child gender.
Main results and the role of chance: In total, there were 472 live birth singletons. Of the 472 singleton pregnancies, 209 were conceived after IUI-OS (136 with FSH and 73 with CC as ovarian stimulation), 138 after IVF (50 after IVF-MNC and 88 after IVF-SET) and 125 were conceived naturally.Singletons conceived following IUI-FSH and IUI-CC both had lower birthweights compared to naturally conceived singletons (adjusted difference IUI-FSH -156.3 g, 95% CI -287.9 to -24.7; IUI-CC -160.3 g, 95% CI -316.7 to -3.8). When we compared IVF-MNC and IVF-SET to naturally conceived singletons, no significant difference was found (adjusted difference IVF-MNC 75.8 g, 95% CI -102.0 to 253.7; IVF-SET -10.6 g, 95% CI -159.2 to 138.1). The mean birthweight percentile was only significantly lower in the IUI-FSH group (-7.0 percentile, 95% CI -13.9 to -0.2). The IUI-CC and IVF-SET group had a lower mean percentile and the IVF-MNC group a higher mean percentile, but these groups were not significant different compared to the naturally conceived group (IUI-CC -5.1 percentile, 95% CI -13.3 to 3.0; IVF-MNC 4.4 percentile, 95% CI -4.9 to 13.6; IVF-SET -1.3 percentile, 95% CI -9.1 to 6.4).Looking at the laboratory process that took place, singletons conceived following IUI-OS had lower birthweights than naturally conceived singletons (adjusted difference -157.7 g, 95% CI -277.4 to -38.0). The IVF group had comparable birthweights with the naturally conceived group (adjusted difference 20.9 g, 95% CI -110.8 to 152.6). The mean birthweight percentile was significantly lower in the IUI-OS group compared to the natural group (-6.4 percentile, 95% CI -12.6 to -0.1). The IVF group was comparable (0.7 percentile, 95% CI -6.1 to 7.6).
Limitations, reasons for caution: The results are limited by the number of cases. The data were collected prospectively alongside the randomized controlled trials, but analyzed as treated.
Wider implications of the findings: Our data suggest IUI in a stimulated cycle may have a negative impact on the birthweight of the child and possibly on pre-eclampsia. Further research should look into the effect of different methods of ovarian stimulation on placenta pathology and pre-eclampsia in couples with unexplained subfertility using naturally conceived singletons in the unexplained population as a reference.
Study funding/competing interest(s): Both initial trials were supported by a grant from ZonMW, the Dutch Organization for Health Research and Development (INeS 120620027, SUPER 80-83600-98-10192). The INeS study also had a grant from Zorgverzekeraars Nederland, the Dutch association of healthcare insurers (09-003). B.W.J.M. is supported by an NHMRC investigator Grant (GNT1176437) and reports consultancy for ObsEva, Merck Merck KGaA, Guerbet and iGenomix, outside the submitted work. A.H. reports grants from Ferring Pharmaceutical company (the Netherlands), outside the submitted work. F.J.M.B. receives monetary compensation as a member of the external advisory board for Merck Serono (the Netherlands), Ferring Pharmaceutics BV (the Netherlands) and Gedeon Richter (Belgium), he receives personal fees from educational activities for Ferring BV (the Netherlands) and for advisory and consultancy work for Roche and he receives research support grants from Merck Serono and Ferring Pharmaceutics BV, outside the submitted work. The remaining authors have nothing to disclose.
Trial registration number: INeS study Trial NL915 (NTR939); SUPER Trial NL3895 (NTR4057).
Keywords: birthweight; laboratory procedures; ovarian stimulation; perinatal outcomes; unexplained subfertility.
© The Author(s) 2020. Published by Oxford University Press on behalf of European Society of Human Reproduction and Embryology.
Figures
References
-
- Bensdorp AJ, Tjon-Kon-Fat RI, Bossuyt PM, Koks CA, Oosterhuis GJ, Hoek A, Hompes PG, Broekmans FJ, Verhoeve HR, de Bruin JP. et al. Prevention of multiple pregnancies in couples with unexplained or mild male subfertility: randomised controlled trial of in vitro fertilisation with single embryo transfer or in vitro fertilisation in modified natural cycle compared with intrauterine insemination with controlled ovarian hyperstimulation. BMJ 2015;350:g7771. - PMC - PubMed
-
- Berntsen S, Soderstrom-Anttila V, Wennerholm UB, Laivuori H, Loft A, Oldereid NB, Romundstad LB, Bergh C, Pinborg A.. The health of children conceived by ART: ‘the chicken or the egg?’. Hum Reprod Update 2019;25:137–158. - PubMed
-
- Chen XK, Wen SW, Bottomley J, Smith GN, Leader A, Walker MC.. In vitro fertilization is associated with an increased risk for preeclampsia. Hypertens Pregnancy 2009;28:1–12. - PubMed
-
- Danhof NA, van Wely M, Repping S, Koks C, Verhoeve HR, de Bruin JP, Verberg MFG, van Hooff MHA, Cohlen BJ, van Heteren CF. et al. ; SUPER Study Group. Follicle stimulating hormone versus clomiphene citrate in intrauterine insemination for unexplained subfertility: a randomized controlled trial. Hum Reprod 2018;33:1866–1874. - PubMed
-
- De Geyter C, Calhaz-Jorge C, Kupka MS, Wyns C, Mocanu E, Motrenko T, Scaravelli G, Smeenk J, Vidakovic S, Goossens V. et al. ART in Europe, 2014: results generated from European registries by ESHRE: the European IVF-monitoring Consortium (EIM) for the European Society of Human Reproduction and Embryology (ESHRE). Hum Reprod 2018;33:1586–1601. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
