

Accuracy and Reproducibility of Intraoperative Assessment on Tumor Spread Through Air Spaces in Stage 1 Lung Adenocarcinomas
- PMID: 33348084
- PMCID: PMC8836021
- DOI: 10.1016/j.jtho.2020.12.005
Accuracy and Reproducibility of Intraoperative Assessment on Tumor Spread Through Air Spaces in Stage 1 Lung Adenocarcinomas
Abstract
Introduction: Tumor spread through air spaces (STAS) is associated with worse prognosis in early-stage lung adenocarcinomas, particularly in sublobar resection. Intraoperative consultation for STAS has been advocated to guide surgical management. However, data on accuracy and reproducibility of intraoperative assessment of STAS remain limited. We evaluated diagnostic yield, interobserver agreement (IOA), and intraobserver agreement (ITA) for STAS detection on frozen section (FS).
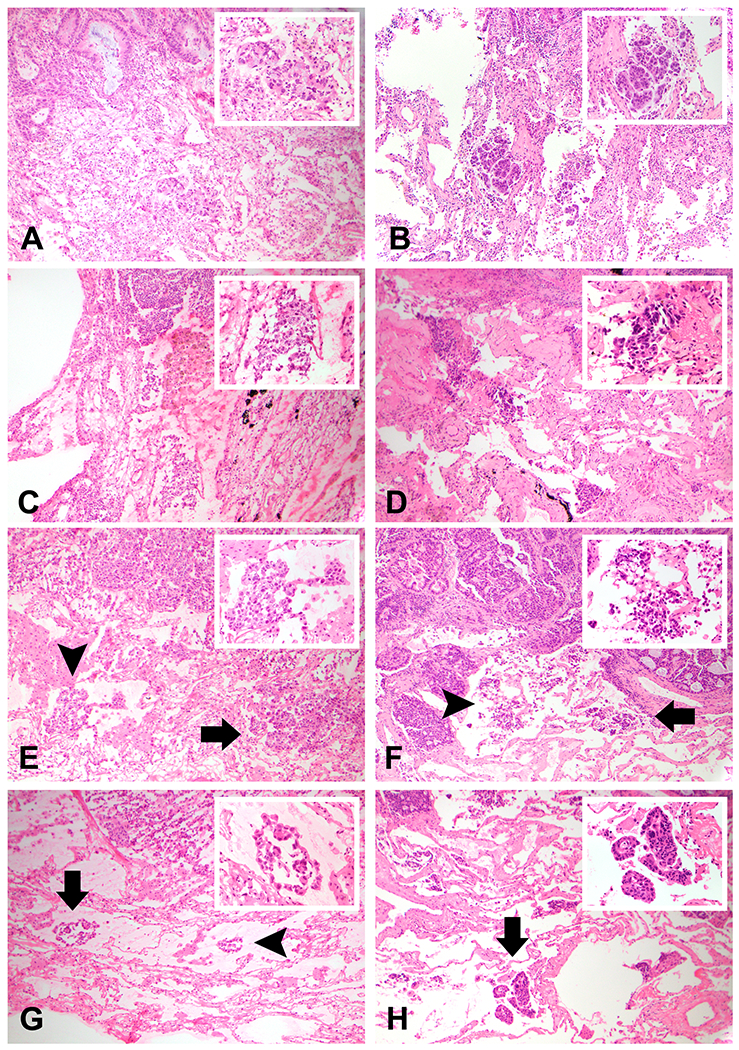
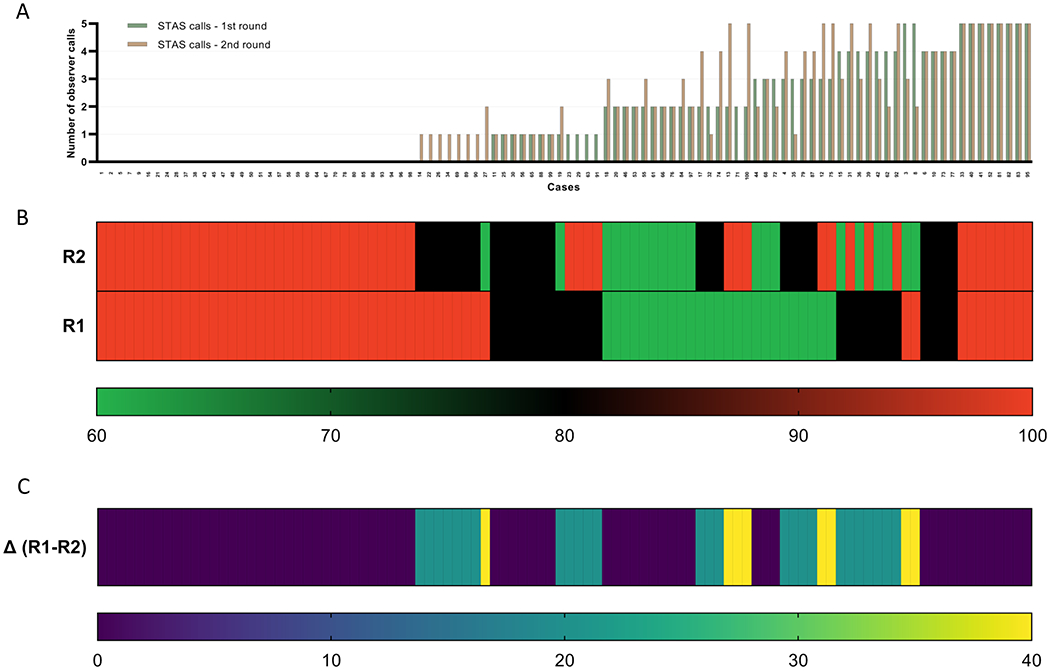
Methods: A panel of three pathologists evaluated stage 1 lung adenocarcinomas (n = 100) for the presence or absence of STAS and artifacts as reference. Five pulmonary pathologists independently reviewed all cases in two rounds, detecting STAS and artifacts in FS and the corresponding FS permanent and non-FS permanent, with a consensus conference between rounds.
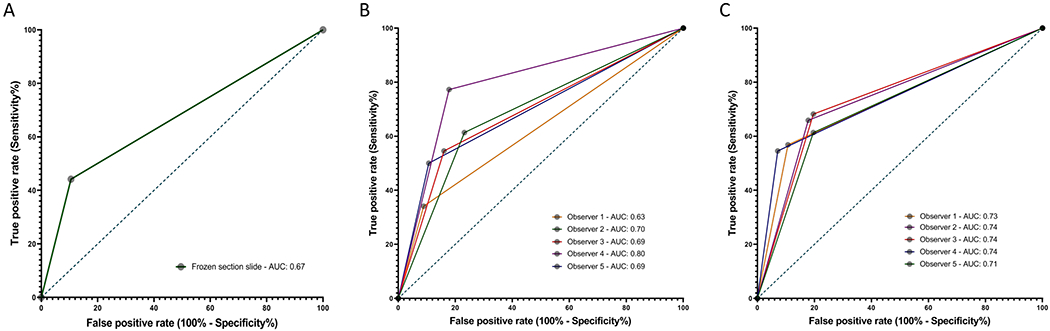
Results: The FS had low sensitivity (44%), high specificity (91%), relatively high accuracy (71%), and overall area under the receiver operating characteristic curve of 0.67 for detecting STAS. The average ITA was moderate for both STAS (κmean: 0.598) and artifact (κmean: 0.402) detection on FS. IOA was moderate for STAS (κround-1: 0.453; κround-2: 0.506) and fair for artifact (κround-1: 0.300; κround-2: 0.204) detection on FS. IOA for STAS improved in FS permanent and non-FS permanent, whereas ITA was similar across section types. On multivariable logistic regression, the only significant predictor of diagnostic discordance was the presence of artifacts.
Conclusions: FS is highly specific but not sensitive for STAS detection in stage 1 lung adenocarcinomas. IOA on STAS is moderate in FS and improved only marginally after a consensus conference, raising concerns regarding global implementation of intraoperative assessment of STAS and warranting more precise criteria for STAS and artifacts.
Keywords: Diagnostic yield; Frozen section; Lung adenocarcinoma; Reproducibility; Tumor spread through air spaces (STAS).
Copyright © 2020 International Association for the Study of Lung Cancer. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Kodama T, Kameya T, Shimosato Y, Koketsu H, Yoneyama T, Tamai S. Cell incohesiveness and pattern of extension in a rare case of bronchioloalveolar carcinoma. Ultrastruct Pathol. 1980. Apr-Jun;1(2):177–88. PMID: 6262967 - PubMed
-
- Kadota K, Nitadori JI, Sima CS, Ujiie H, Rizk NP, Jones DR, et al. Tumor Spread through Air Spaces is an Important Pattern of Invasion and Impacts the Frequency and Location of Recurrences after Limited Resection for Small Stage I Lung Adenocarcinomas. J Thorac Oncol. 2015. May;10(5):806–814. PMID: 25629637 - PMC - PubMed
-
- Thunnissen E, Blaauwgeers HJ, de Cuba EM, Yick CY, Flieder DB. Ex Vivo Artifacts and Histopathologic Pitfalls in the Lung. Arch Pathol Lab Med. 2016. Mar;140(3):212–20. - PubMed
-
- Travis WD, Brambilla E, Nicholson AG, Yatabe Y, Austin JHM, Beasley MB, et al. The 2015 World Health Organization Classification of Lung Tumors: Impact of Genetic, Clinical and Radiologic Advances Since the 2004 Classification. J Thorac Oncol. 2015. Sep;10(9):1243–1260. PMID: 26291008 - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
