

Gastroschisis: A State-of-the-Art Review
- PMID: 33348575
- PMCID: PMC7765881
- DOI: 10.3390/children7120302
Gastroschisis: A State-of-the-Art Review
Abstract
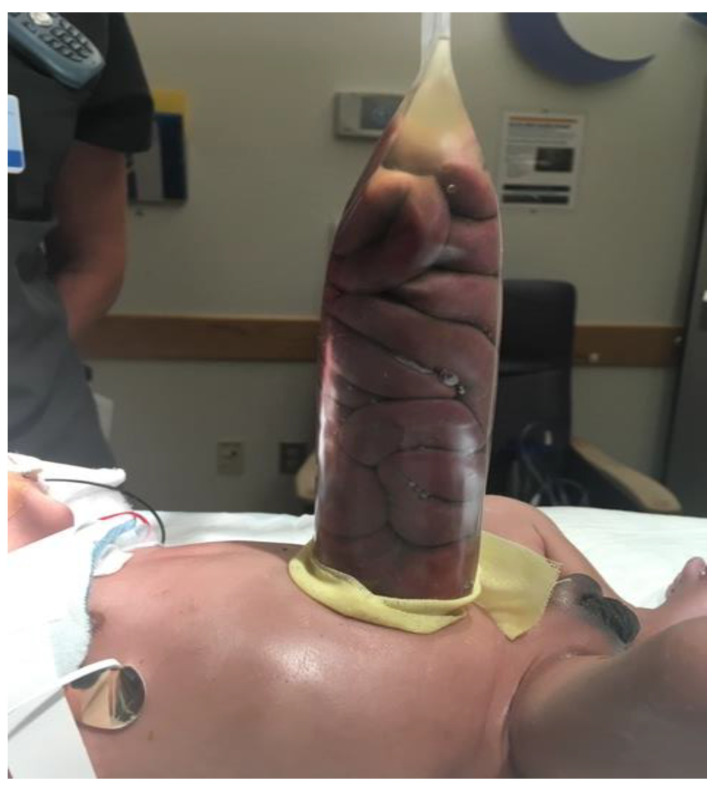
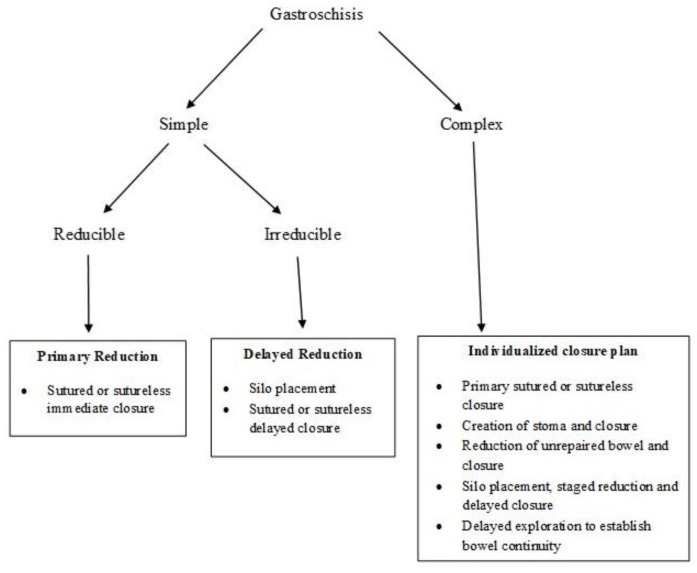
Gastroschisis, the most common type of abdominal wall defect, has seen a steady increase in its prevalence over the past several decades. It is identified, both prenatally and postnatally, by the location of the defect, most often to the right of a normally-inserted umbilical cord. It disproportionately affects young mothers, and appears to be associated with environmental factors. However, the contribution of genetic factors to the overall risk remains unknown. While approximately 10% of infants with gastroschisis have intestinal atresia, extraintestinal anomalies are rare. Prenatal ultrasound scans are useful for early diagnosis and identification of features that predict a high likelihood of associated bowel atresia. The timing and mode of delivery for mothers with fetuses with gastroschisis have been somewhat controversial, but there is no convincing evidence to support routine preterm delivery or elective cesarean section in the absence of obstetric indications. Postnatal surgical management is dictated by the condition of the bowel and the abdominal domain. The surgical options include either primary reduction and closure or staged reduction with placement of a silo followed by delayed closure. The overall prognosis for infants with gastroschisis, in terms of both survival as well as long-term outcomes, is excellent. However, the management and outcomes of a subset of infants with complex gastroschisis, especially those who develop short bowel syndrome (SBS), remains challenging. Future research should be directed towards identification of epidemiological factors contributing to its rising incidence, improvement in the management of SBS, and obstetric/fetal interventions to minimize intestinal damage.
Keywords: abdominal defect; congenital anomaly; infant; newborn; nutrition.
Conflict of interest statement
The authors declare no conflict of interest.
Figures



References
-
- Moore T.C., Stokes G.E. Gastroschisis; Report of two cases treated by a modification of the gross operation for omphalocele. Surgery. 1953;33:112–120. - PubMed
-
- International Clearinghouse for Birth Defects Surveillance and Research Annual Report 2014. International Centre on Birth Defects (ICBDSR Centre), Rome, Italy. [(accessed on 4 August 2020)]; Available online: http://www.icbdsr.org/wp-content/annual_report/Report2014.pdf.
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
