

The Use of a Kinetic Therapy Rotational Bed in Pediatric Acute Respiratory Distress Syndrome: A Case Series
- PMID: 33348617
- PMCID: PMC7766378
- DOI: 10.3390/children7120303
The Use of a Kinetic Therapy Rotational Bed in Pediatric Acute Respiratory Distress Syndrome: A Case Series
Abstract
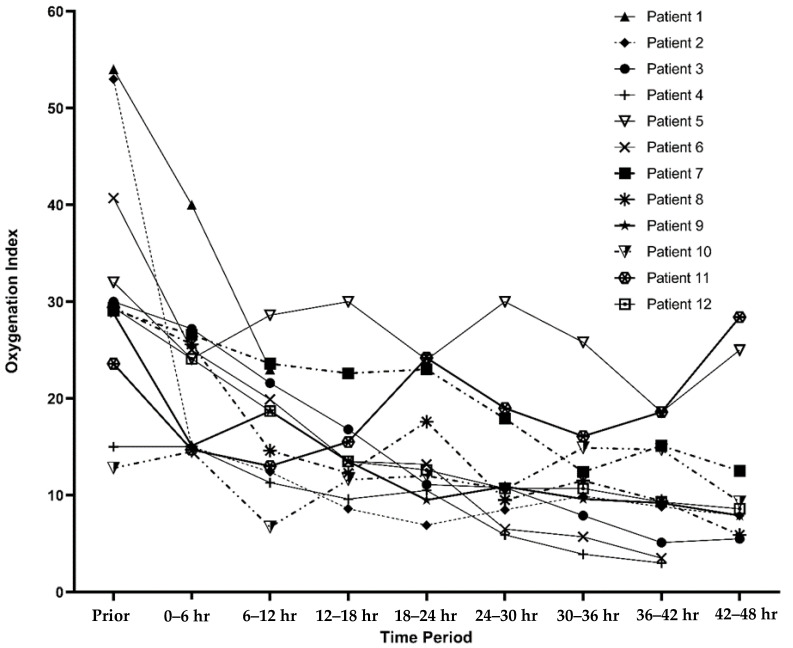
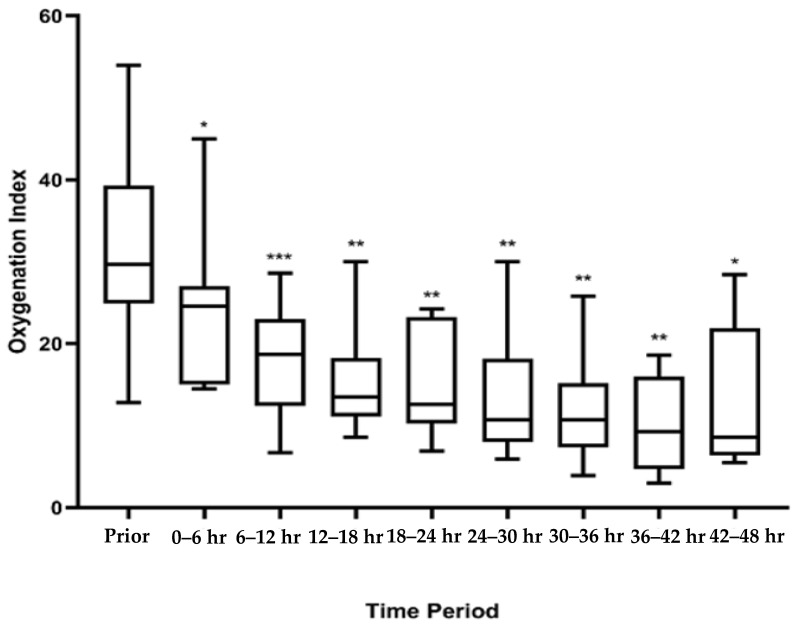
Patients with acute respiratory distress syndrome (ARDS) commonly have dependent atelectasis and heterogeneous lung disease. Due to the heterogenous lung volumes seen, the application of positive end expiratory pressure (PEEP) can have both beneficial and deleterious effects. Alternating supine and prone positioning may be beneficial in ARDS by providing more homogenous distribution of PEEP and decreasing intrapulmonary shunt. In pediatrics, the pediatric acute lung injury and consensus conference (PALICC) recommended to consider it in severe pediatric ARDS (PARDS). Manually prone positioning patients can be burdensome in larger patients. In adults, the use of rotational beds has eased care of these patients. There is little published data about rotational bed therapy in children. Therefore, we sought to describe the use of a rotational bed in children with PARDS. We performed a retrospective case series of children who utilized a rotational bed as an adjunctive therapy for their PARDS. Patient data were collected and analyzed. Descriptive statistical analyses were performed and reported. Oxygenation indices (OI) pre- and post-prone positioning were analyzed. Twelve patients with PARDS were treated with a rotational bed with minimal adverse events. There were no complications noted. Three patients had malfunctioning of their arterial line while on the rotational bed. Oxygenation indices improved over time in 11 of the 12 patients included in the study while on the rotational bed. Rotational beds can be safely utilized in pediatric patients. In larger children with PARDS, where it may be more difficult to perform a manual prone position, use of a rotational bed can be considered a safe alternative.
Keywords: Intensive care units; acute respiratory distress syndrome; artificial respiration; critical illness; pediatrics; prone position.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Puybasset L., Gusman P., Muller J.C., Cluzel P., Coriat P., Rouby J.J. Regional distribution of gas and tissue in acute respiratory distress syndrome. III. Consequences for the effects of positive end-expiratory pressure. CT Scan ARDS Study Group. Adult Respiratory Distress Syndrome. Intensive Care Med. 2000;26:1215–1227. doi: 10.1007/s001340051340. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
