

Effects of Juvenile or Adolescent Working Memory Experience and Inter-Alpha Inhibitor Protein Treatment after Neonatal Hypoxia-Ischemia
- PMID: 33348631
- PMCID: PMC7765798
- DOI: 10.3390/brainsci10120999
Effects of Juvenile or Adolescent Working Memory Experience and Inter-Alpha Inhibitor Protein Treatment after Neonatal Hypoxia-Ischemia
Abstract
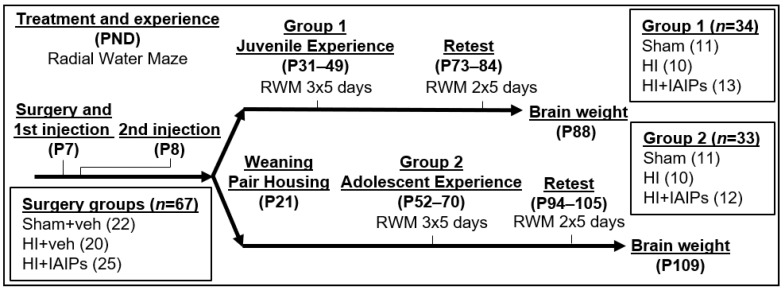
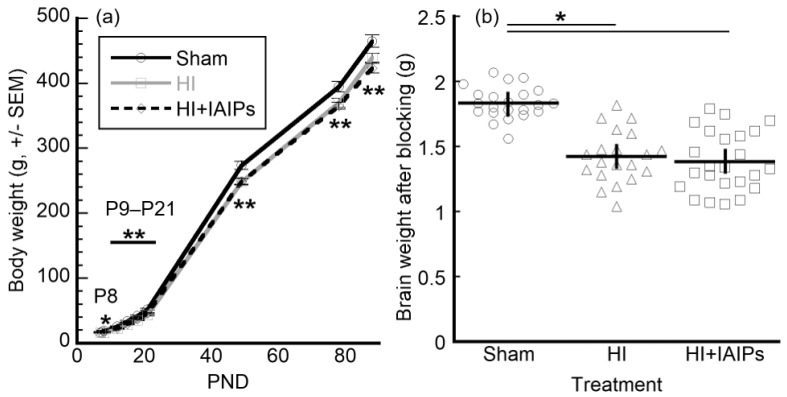
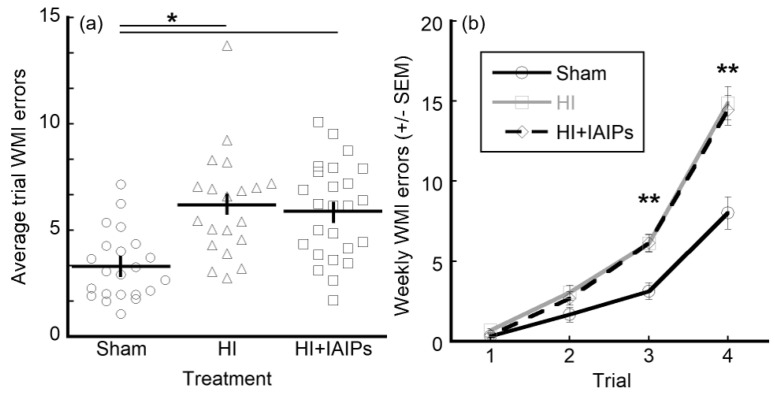
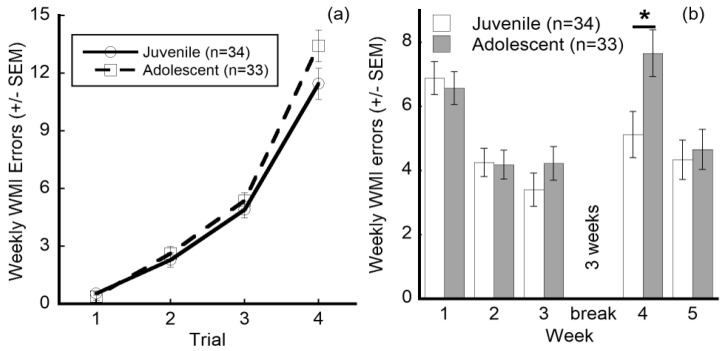
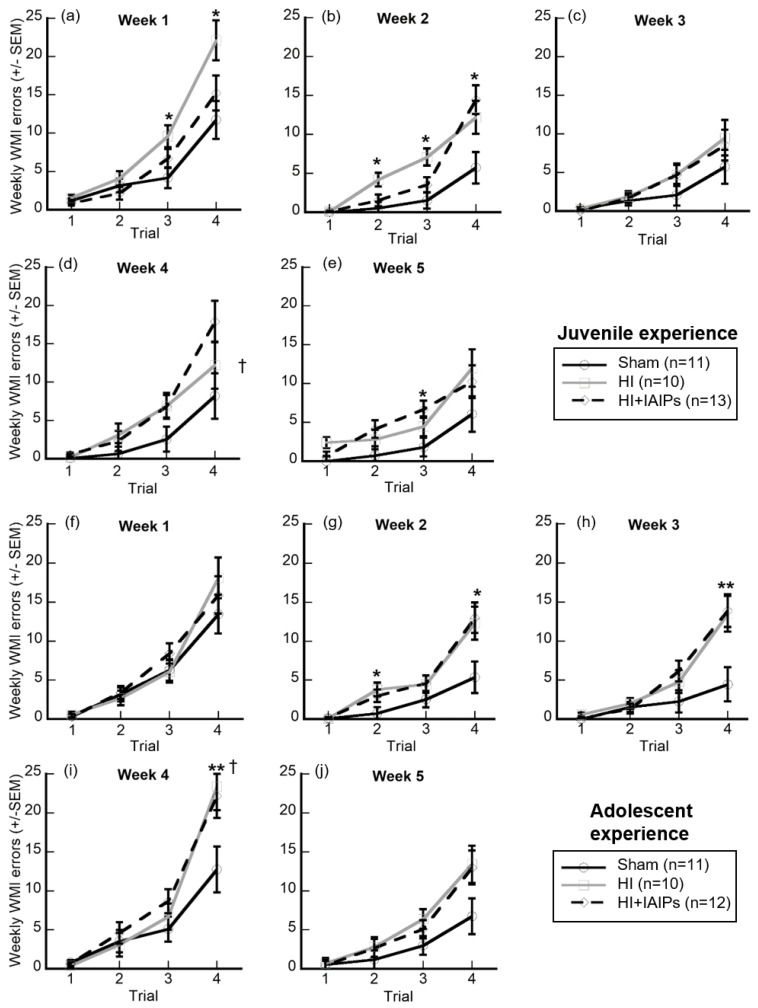
Hypoxic-Ischemic (HI) brain injury in the neonate contributes to life-long cognitive impairment. Early diagnosis and therapeutic interventions are critical but limited. We previously reported in a rat model of HI two interventional approaches that improve cognitive and sensory function: administration of Inter-alpha Inhibitor Proteins (IAIPs) and early experience in an eight-arm radial water maze (RWM) task. Here, we expanded these studies to examine the combined effects of IAIPs and multiple weeks of RWM assessment beginning with juvenile or adolescent rats to evaluate optimal age windows for behavioral interventions. Subjects were divided into treatment groups; HI with vehicle, sham surgery with vehicle, and HI with IAIPs, and received either juvenile (P31 initiation) or adolescent (P52 initiation) RWM testing, followed by adult retesting. Error rates on the RWM decreased across weeks for all conditions. Whereas, HI injury impaired global performance as compared to shams. IAIP-treated HI subjects tested as juveniles made fewer errors as compared to their untreated HI counterparts. The juvenile group made significantly fewer errors on moderate demand trials and showed improved retention as compared to the adolescent group during the first week of adult retesting. Together, results support and extend our previous findings that combining behavioral and anti-inflammatory interventions in the presence of HI improves subsequent learning performance. Results further indicate sensitive periods for behavioral interventions to improve cognitive outcomes. Specifically, early life cognitive experience can improve long-term learning performance even in the presence of HI injury. Results from this study provide insight into typical brain development and the impact of developmentally targeted therapeutics and task-specific experience on subsequent cognitive processing.
Keywords: Inter-alpha Inhibitor Proteins; early behavioral intervention; eight-arm water maze; encephalopathy; hypoxia-ischemia; immune modulator; inflammation; working memory.
Conflict of interest statement
Yow Pin Lim is employed by ProThera Biologics, Inc. and has a significant financial stake in the company. All other authors declare no conflicts of interest and that they have no competing interests.
Figures
Similar articles
-
Effects of age, experience and inter-alpha inhibitor proteins on working memory and neuronal plasticity after neonatal hypoxia-ischemia.Behav Brain Res. 2016 Apr 1;302:88-99. doi: 10.1016/j.bbr.2016.01.016. Epub 2016 Jan 8. Behav Brain Res. 2016. PMID: 26778784 Free PMC article.
-
Neuroprotective effects of inter-alpha inhibitor proteins after hypoxic-ischemic brain injury in neonatal rats.Exp Neurol. 2019 Jul;317:244-259. doi: 10.1016/j.expneurol.2019.03.013. Epub 2019 Mar 23. Exp Neurol. 2019. PMID: 30914159 Free PMC article.
-
Effects of inter-alpha inhibitor proteins on neonatal brain injury: Age, task and treatment dependent neurobehavioral outcomes.Exp Neurol. 2014 Nov;261:424-33. doi: 10.1016/j.expneurol.2014.07.012. Epub 2014 Jul 30. Exp Neurol. 2014. PMID: 25084519 Free PMC article.
-
Alterations in inter-alpha inhibitor protein expression after hypoxic-ischemic brain injury in neonatal rats.Int J Dev Neurosci. 2018 Apr;65:54-60. doi: 10.1016/j.ijdevneu.2017.10.008. Epub 2017 Oct 25. Int J Dev Neurosci. 2018. PMID: 29079121 Free PMC article.
-
Effects of inter-alpha inhibitor proteins on brain injury after exposure of neonatal rats to severe hypoxia-ischemia.Exp Neurol. 2020 Dec;334:113442. doi: 10.1016/j.expneurol.2020.113442. Epub 2020 Sep 5. Exp Neurol. 2020. PMID: 32896573 Free PMC article.
Cited by
-
Importance of Control Groups for Evaluating Long-Term Behavioral and Cognitive Outcomes of Controlled Cortical Impact in Immature Rats.J Neurotrauma. 2023 Jun;40(11-12):1197-1215. doi: 10.1089/neu.2021.0376. Epub 2023 Mar 1. J Neurotrauma. 2023. PMID: 36416234 Free PMC article.
-
Inter-alpha Inhibitor Proteins Ameliorate Brain Injury and Improve Behavioral Outcomes in a Sex-Dependent Manner After Exposure to Neonatal Hypoxia Ischemia in Newborn and Young Adult Rats.Neurotherapeutics. 2022 Mar;19(2):528-549. doi: 10.1007/s13311-022-01217-8. Epub 2022 Mar 15. Neurotherapeutics. 2022. PMID: 35290609 Free PMC article.
-
A systematic review of immune-based interventions for perinatal neuroprotection: closing the gap between animal studies and human trials.J Neuroinflammation. 2023 Oct 20;20(1):241. doi: 10.1186/s12974-023-02911-w. J Neuroinflammation. 2023. PMID: 37864272 Free PMC article.
References
Grants and funding
LinkOut - more resources
Full Text Sources
