

Qualitative and Quantitative Wall Enhancement on Magnetic Resonance Imaging Is Associated With Symptoms of Unruptured Intracranial Aneurysms
- PMID: 33349014
- PMCID: PMC7770055
- DOI: 10.1161/STROKEAHA.120.029685
Qualitative and Quantitative Wall Enhancement on Magnetic Resonance Imaging Is Associated With Symptoms of Unruptured Intracranial Aneurysms
Abstract
Background and purpose: Aneurysmal wall enhancement (AWE) on vessel wall magnetic resonance imaging (VW-MRI) has been described as a new imaging biomarker of unstable unruptured intracranial aneurysms (UIAs). Previous studies of symptomatic UIAs are limited due to small sample sizes and lack of AWE quantification. Our study aims to investigate whether qualitative and quantitative assessment of AWE can differentiate symptomatic and asymptomatic UIAs.
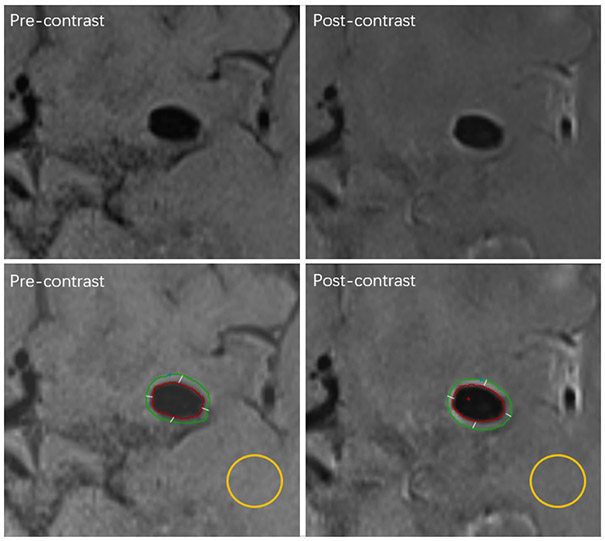
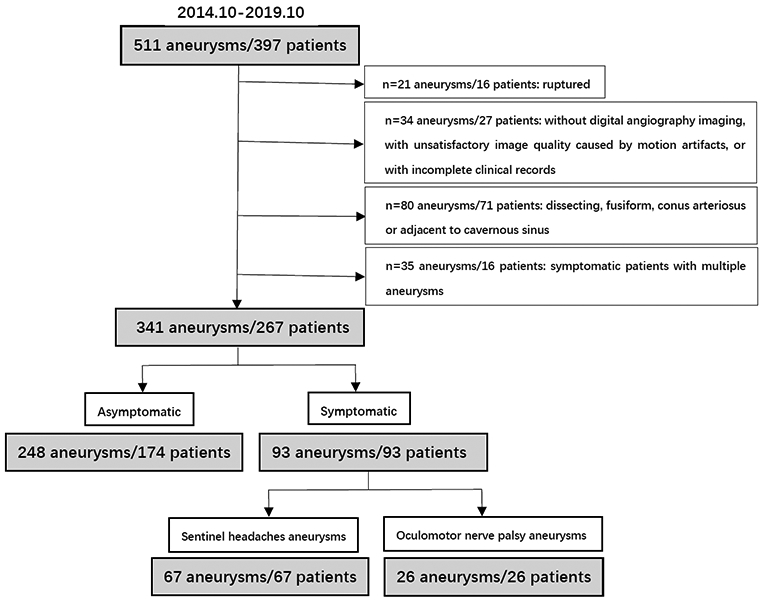
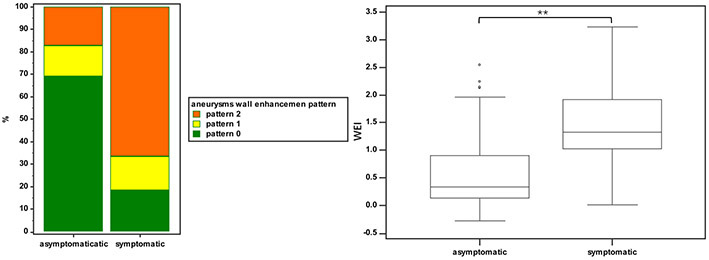
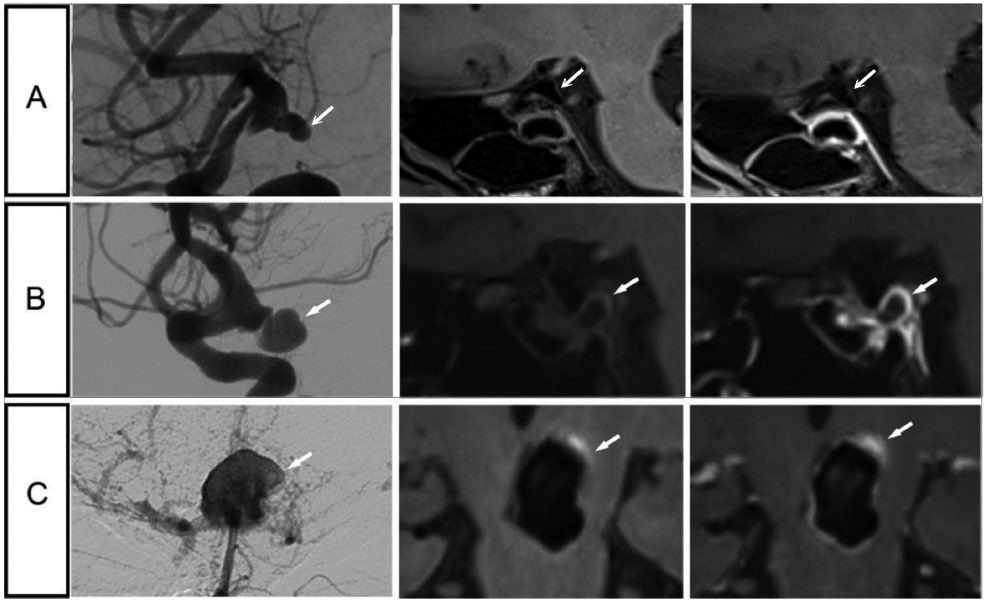
Methods: Consecutive patients with UIAs were prospectively recruited for vessel wall magnetic resonance imaging at 3T from October 2014 to October 2019. UIAs were categorized as symptomatic if presenting with sentinel headache or oculomotor nerve palsy directly related to the aneurysm. Evaluation of wall enhancement included enhancement pattern (0=none, 1=focal, and 2=circumferential) and quantitative wall enhancement index (WEI). Univariate and multivariate analyses were used to identify the parameters associated with symptoms.
Results: Two hundred sixty-seven patients with 341 UIAs (93 symptomatic and 248 asymptomatic) were included in this study. Symptomatic UIAs more frequently showed circumferential AWE than asymptomatic UIAs (66.7% versus 17.3%, P<0.001), as well as higher WEI (median [interquartile range], 1.3 [1.0-1.9] versus 0.3 [0.1-0.9], P<0.001). In multivariate analysis, both AWE pattern and WEI were independent factors associated with symptoms (odds ratio=2.03 across AWE patterns [95% CI, 1.21-3.39], P=0.01; odds ratio=3.32 for WEI [95% CI, 1.51-7.26], P=0.003). The combination of AWE pattern and WEI had an area under the curve of 0.91 to identify symptomatic UIAs, with a sensitivity of 95.7% and a specificity of 73.4%.
Conclusions: In a large cohort of UIAs with vessel wall magnetic resonance imaging, both AWE pattern and WEI were independently associated with aneurysm-related symptoms. The qualitative and quantitative features of AWE can potentially be used to identify unstable intracranial aneurysms.
Keywords: biomarkers; headache; inflammation; intracranial aneurysm; magnetic resonance imaging.
Figures
References
-
- Vernooij MW, Ikram MA, Tanghe HL, Vincent AJ, Hofman A, Krestin GP, Niessen WJ, Breteler MM, van der Lugt A. Incidental findings on brain mri in the general population. N Engl J Med. 2007;357:1821–1828 - PubMed
-
- Gilard V, Grangeon L, Guegan-Massardier E, Sallansonnet-Froment M, Maltete D, Derrey S, Proust F. Headache changes prior to aneurysmal rupture: A symptom of unruptured aneurysm? Neurochirurgie. 2016;62:241–244 - PubMed
-
- Yanaka K, Matsumaru Y, Mashiko R, Hyodo A, Sugimoto K, Nose T. Small unruptured cerebral aneurysms presenting with oculomotor nerve palsy. Neurosurgery. 2003;52:553–557; discussion 556-557 - PubMed
-
- Gaberel T, Borha A, di Palma C, Emery E. Clipping versus coiling in the management of posterior communicating artery aneurysms with third nerve palsy: A systematic review and meta-analysis. World Neurosurg. 2016;87:498–506 e494 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
