

Association of First Primary Cancer With Risk of Subsequent Primary Cancer Among Survivors of Adult-Onset Cancers in the United States
- PMID: 33351041
- PMCID: PMC7756242
- DOI: 10.1001/jama.2020.23130
Association of First Primary Cancer With Risk of Subsequent Primary Cancer Among Survivors of Adult-Onset Cancers in the United States
Erratum in
-
Incorrect Figure Data.JAMA. 2021 May 18;325(19):2020. doi: 10.1001/jama.2021.6322. JAMA. 2021. PMID: 33861308 Free PMC article. No abstract available.
Abstract
Importance: The number of cancer survivors who develop new cancers is projected to increase, but comprehensive data on the risk of subsequent primary cancers (SPCs) among survivors of adult-onset cancers are limited.
Objective: To quantify the overall and cancer type-specific risks of SPCs among adult-onset cancer survivors by first primary cancer (FPC) types and sex.
Design, setting, and participants: A retrospective cohort study from 12 Surveillance, Epidemiology, and End Results registries in the United States, that included 1 537 101 persons aged 20 to 84 years diagnosed with FPCs from 1992-2011 (followed up until December 31, 2017) and who survived at least 5 years.
Exposures: First primary cancer.
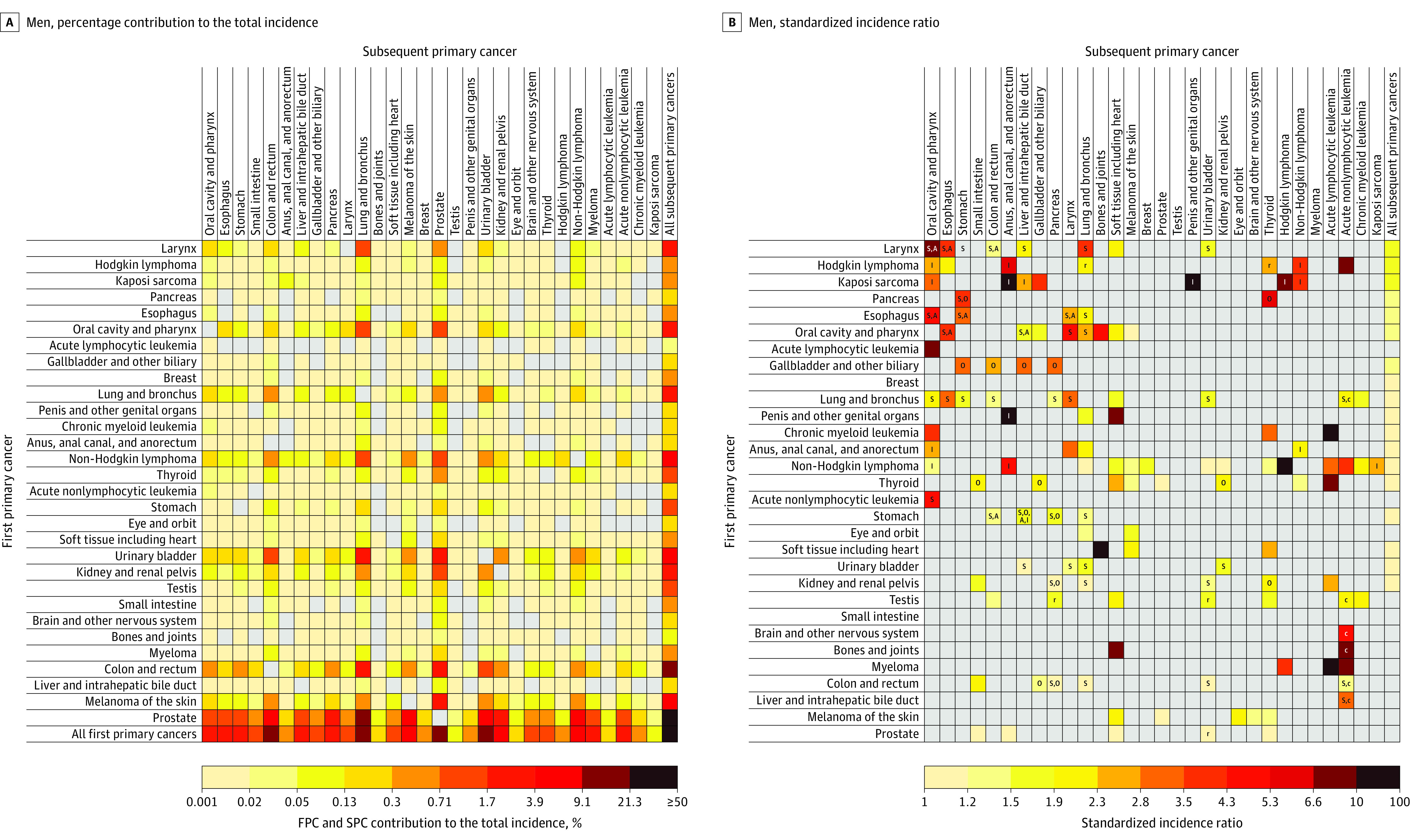
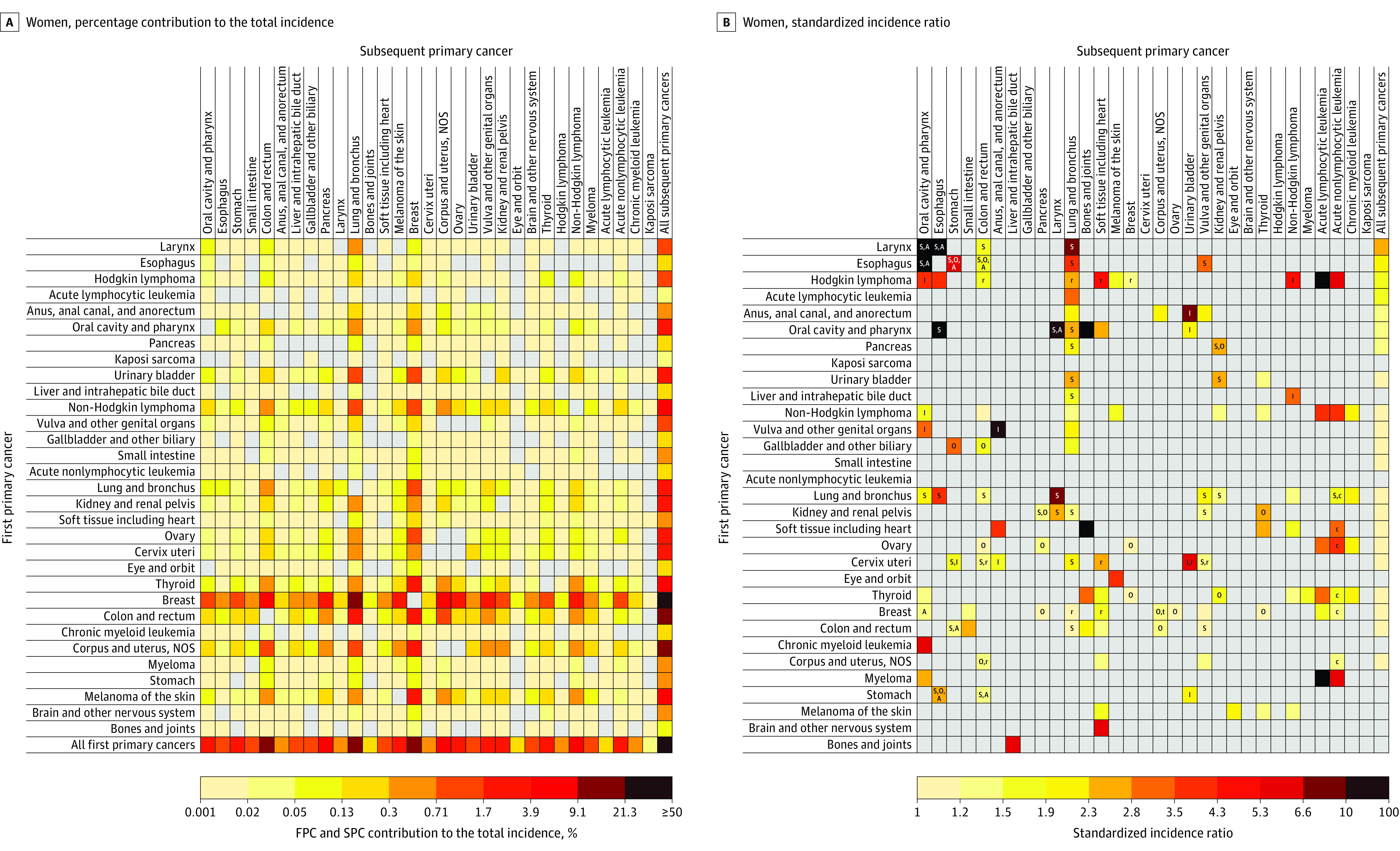
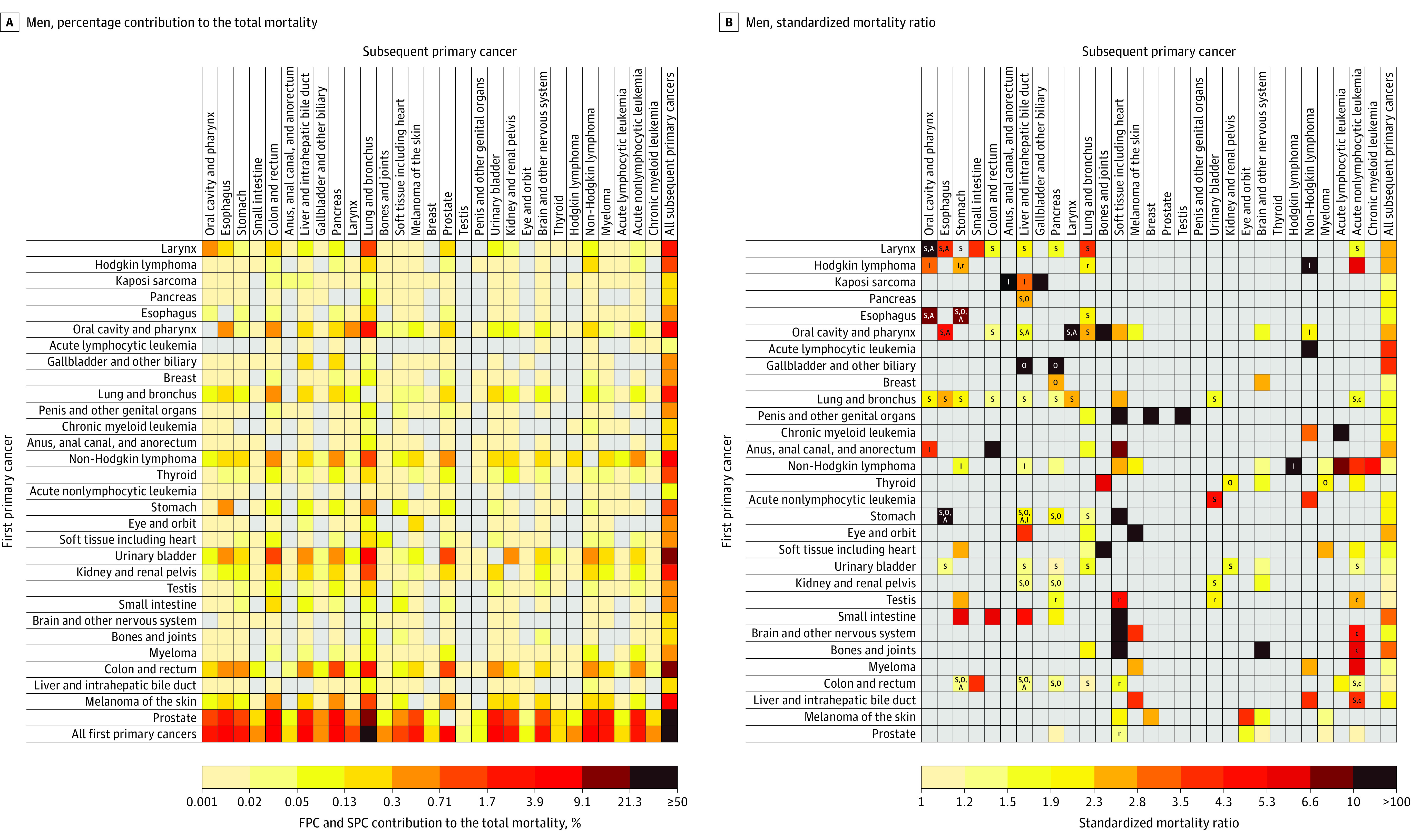
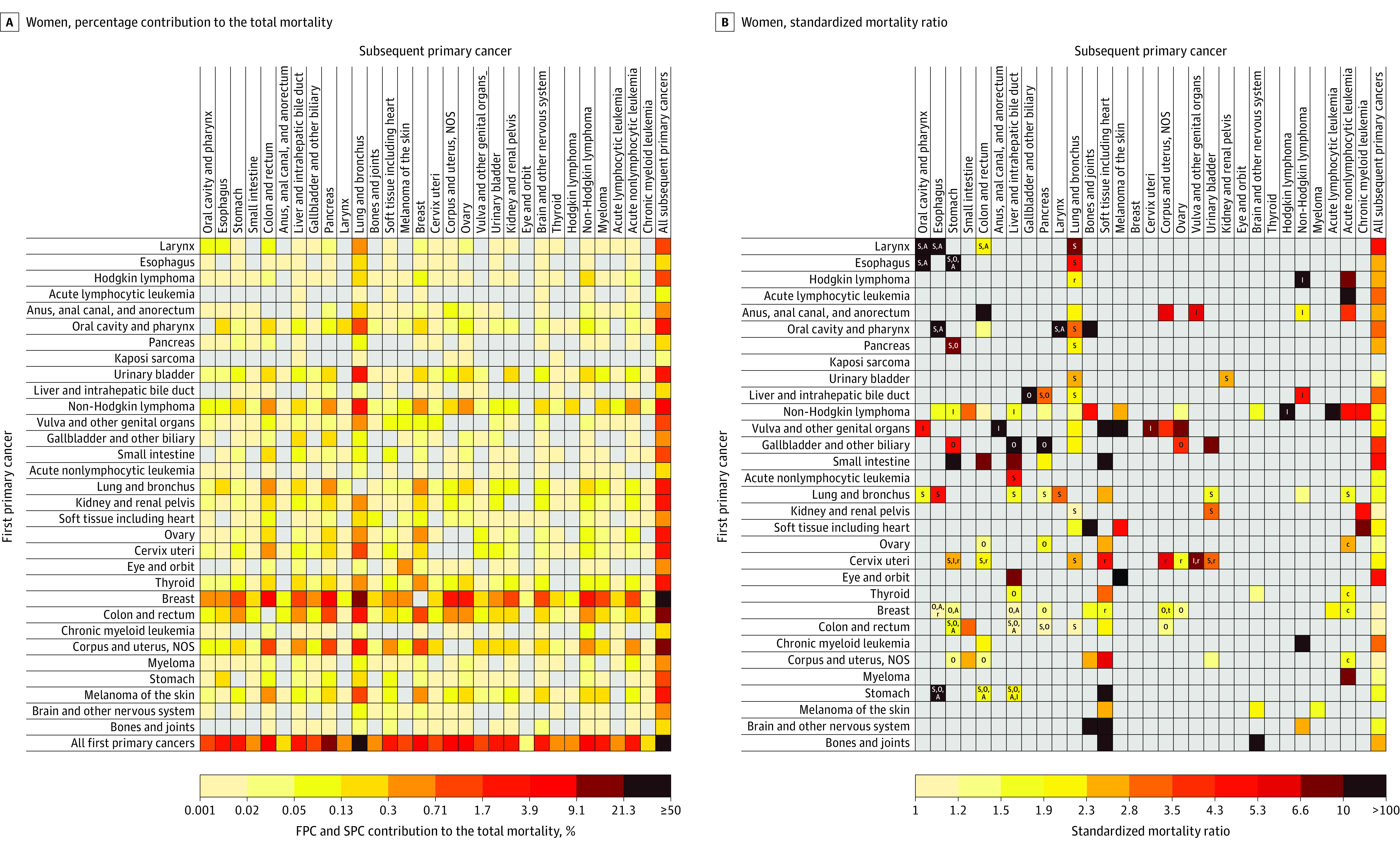
Main outcomes and measures: Incidence and mortality of SPCs per 10 000 person-years; standardized incidence ratio (SIR) and standardized mortality ratio (SMR) compared with those expected in the general population.
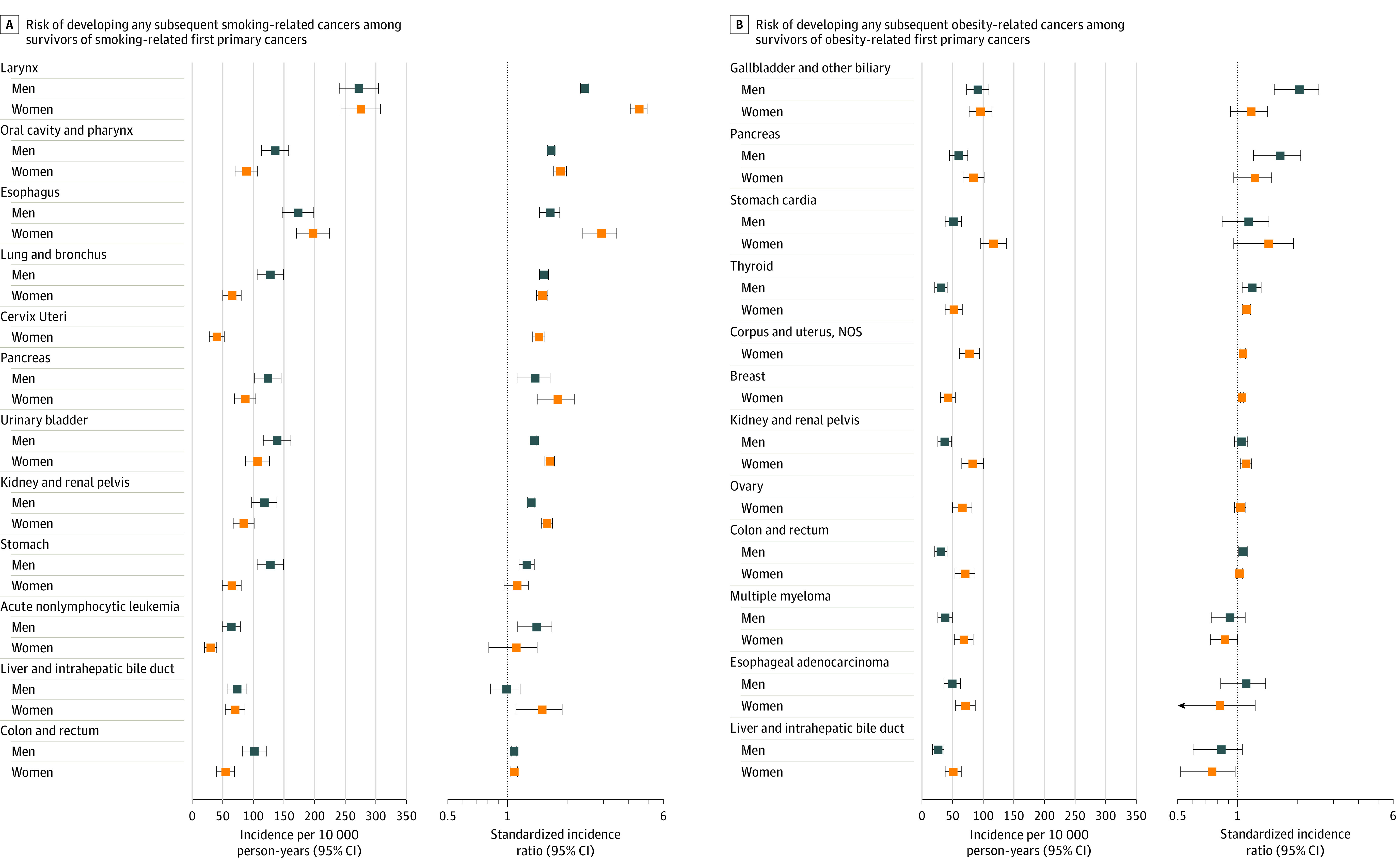
Results: Among 1 537 101 survivors (mean age, 60.4 years; 48.8% women), 156 442 SPC cases and 88 818 SPC deaths occurred during 11 197 890 person-years of follow-up (mean, 7.3 years). Among men, the overall risk of developing any SPCs was statistically significantly higher for 18 of the 30 FPC types, and risk of dying from any SPCs was statistically significantly higher for 27 of 30 FPC types as compared with risks in the general population. Among women, the overall risk of developing any SPCs was statistically significantly higher for 21 of the 31 FPC types, and risk of dying from any SPCs was statistically significantly higher for 28 of 31 FPC types as compared with risks in the general population. The highest overall SIR and SMR were estimated among survivors of laryngeal cancer (SIR, 1.75 [95% CI, 1.68-1.83]; incidence, 373 per 10 000 person-years) and gallbladder cancer (SMR, 3.82 [95% CI, 3.31-4.39]; mortality, 341 per 10 000 person-years) among men, and among survivors of laryngeal cancer (SIR, 2.48 [95% CI, 2.27-2.72]; incidence, 336 per 10 000 person-years; SMR, 4.56 [95% CI, 4.11-5.06]; mortality, 268 per 10 000 person-years) among women. Substantial variation existed in the associations of specific types of FPCs with specific types of SPC risk; however, only a few smoking- or obesity-associated SPCs, such as lung, urinary bladder, oral cavity/pharynx, colorectal, pancreatic, uterine corpus, and liver cancers constituted considerable proportions of the total incidence and mortality, with lung cancer alone accounting for 31% to 33% of mortality from all SPCs.
Conclusions and relevance: Among survivors of adult-onset cancers in the United States, several types of primary cancer were significantly associated with greater risk of developing and dying from an SPC, compared with the general population. Cancers associated with smoking or obesity comprised substantial proportions of overall SPC incidence and mortality among all survivors and highlight the importance of ongoing surveillance and efforts to prevent new cancers among survivors.
Conflict of interest statement
Figures
Comment in
-
Incorporating the Risk for Subsequent Primary Cancers Into the Care of Adult Cancer Survivors: Moving Beyond 5-Year Survival.JAMA. 2020 Dec 22;324(24):2493-2495. doi: 10.1001/jama.2020.23410. JAMA. 2020. PMID: 33351026 No abstract available.
-
Lifestyle Factors Can Lead to Multiple Cancers Over a Lifetime-Here We Go Again.JAMA Oncol. 2021 Apr 1;7(4):505-506. doi: 10.1001/jamaoncol.2020.7360. JAMA Oncol. 2021. PMID: 33351067 No abstract available.
References
-
- Curtis RE, Freedman DM, Ron E, et al. , eds. New Malignancies Among Cancer Survivors: SEER Cancer Registries, 1973-2000. National Cancer Institute; 2006. NIH publication 05-5302.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
