

Assessment of Maternal and Neonatal SARS-CoV-2 Viral Load, Transplacental Antibody Transfer, and Placental Pathology in Pregnancies During the COVID-19 Pandemic
- PMID: 33351086
- PMCID: PMC7756241
- DOI: 10.1001/jamanetworkopen.2020.30455
Assessment of Maternal and Neonatal SARS-CoV-2 Viral Load, Transplacental Antibody Transfer, and Placental Pathology in Pregnancies During the COVID-19 Pandemic
Abstract
Importance: Biological data are lacking with respect to risk of vertical transmission and mechanisms of fetoplacental protection in maternal severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection.
Objective: To quantify SARS-CoV-2 viral load in maternal and neonatal biofluids, transplacental passage of anti-SARS-CoV-2 antibody, and incidence of fetoplacental infection.
Design, setting, and participants: This cohort study was conducted among pregnant women presenting for care at 3 tertiary care centers in Boston, Massachusetts. Women with reverse transcription-polymerase chain reaction (RT-PCR) results positive for SARS-CoV-2 were recruited from April 2 to June 13, 2020, and follow-up occurred through July 10, 2020. Contemporaneous participants without SARS-CoV-2 infection were enrolled as a convenience sample from pregnant women with RT-PCR results negative for SARS-CoV-2.
Exposures: SARS-CoV-2 infection in pregnancy, defined by nasopharyngeal swab RT-PCR.
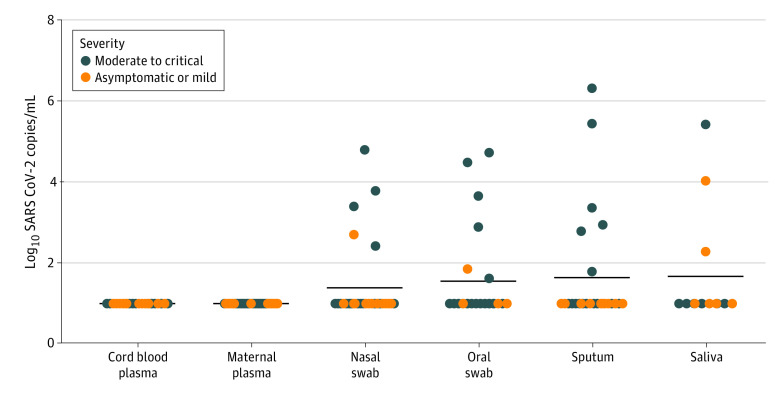
Main outcomes and measures: The main outcomes were SARS-CoV-2 viral load in maternal plasma or respiratory fluids and umbilical cord plasma, quantification of anti-SARS-CoV-2 antibodies in maternal and cord plasma, and presence of SARS-CoV-2 RNA in the placenta.
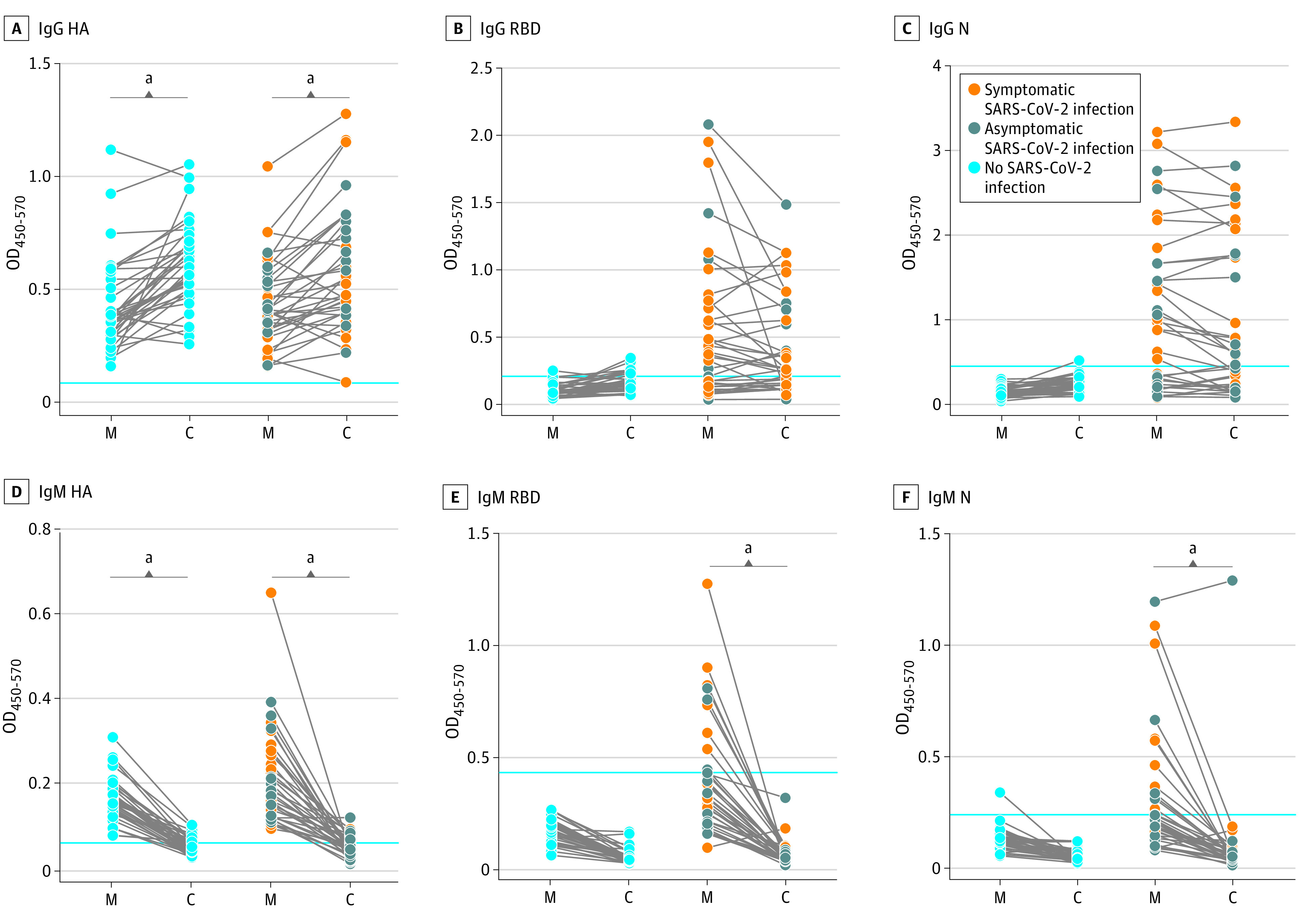
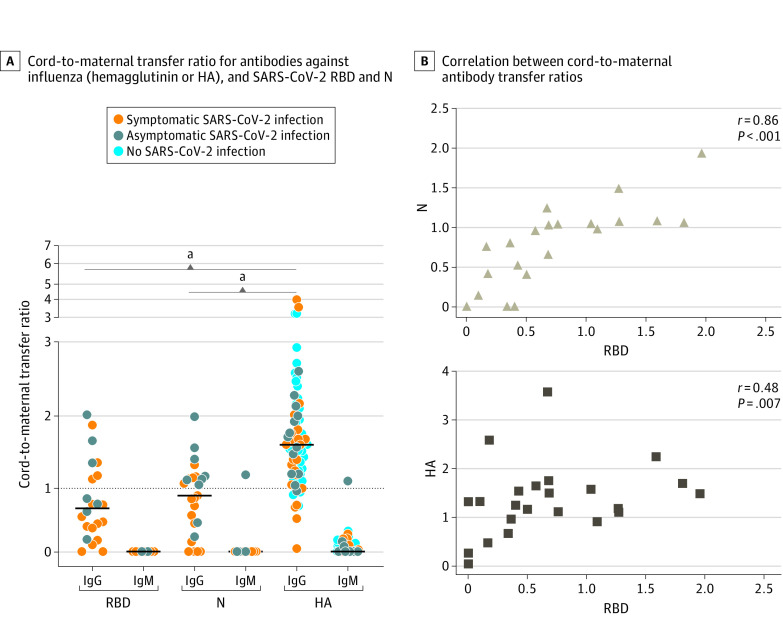
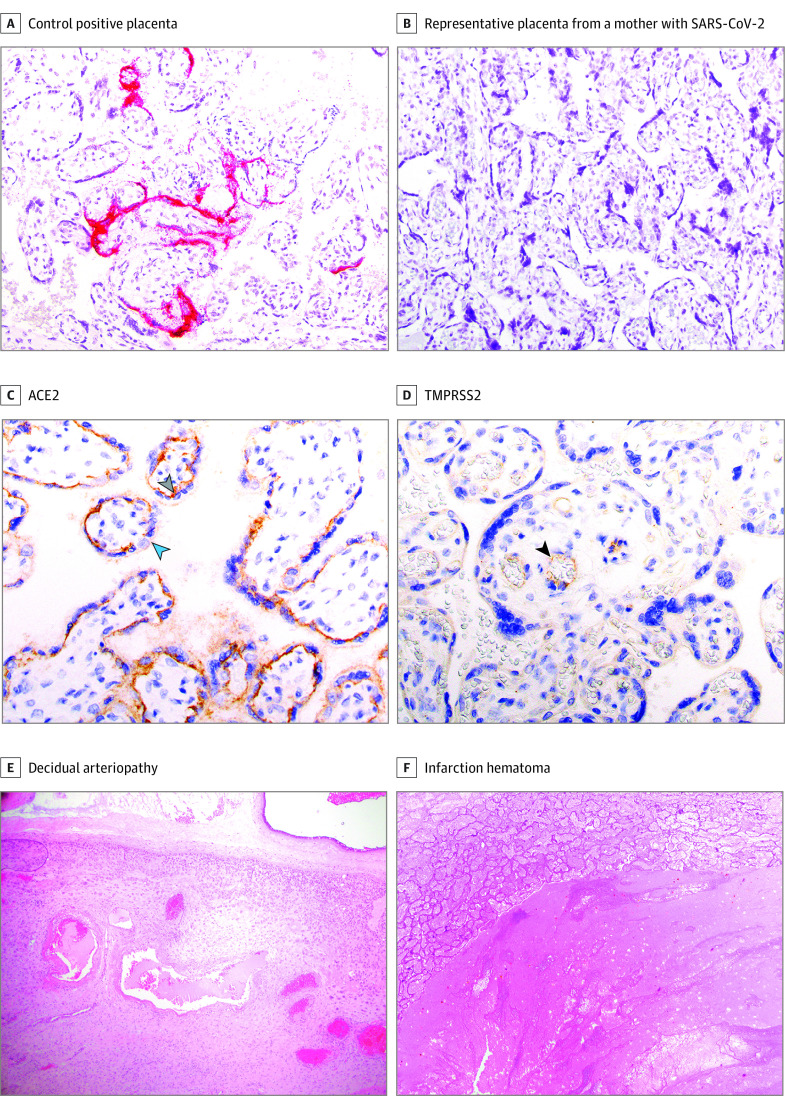
Results: Among 127 pregnant women enrolled, 64 with RT-PCR results positive for SARS-CoV-2 (mean [SD] age, 31.6 [5.6] years) and 63 with RT-PCR results negative for SARS-CoV-2 (mean [SD] age, 33.9 [5.4] years) provided samples for analysis. Of women with SARS-CoV-2 infection, 23 (36%) were asymptomatic, 22 (34%) had mild disease, 7 (11%) had moderate disease, 10 (16%) had severe disease, and 2 (3%) had critical disease. In viral load analyses among 107 women, there was no detectable viremia in maternal or cord blood and no evidence of vertical transmission. Among 77 neonates tested in whom SARS-CoV-2 antibodies were quantified in cord blood, 1 had detectable immunoglobuilin M to nucleocapsid. Among 88 placentas tested, SARS-CoV-2 RNA was not detected in any. In antibody analyses among 37 women with SARS-CoV-2 infection, anti-receptor binding domain immunoglobin G was detected in 24 women (65%) and anti-nucleocapsid was detected in 26 women (70%). Mother-to-neonate transfer of anti-SARS-CoV-2 antibodies was significantly lower than transfer of anti-influenza hemagglutinin A antibodies (mean [SD] cord-to-maternal ratio: anti-receptor binding domain immunoglobin G, 0.72 [0.57]; anti-nucleocapsid, 0.74 [0.44]; anti-influenza, 1.44 [0.80]; P < .001). Nonoverlapping placental expression of SARS-CoV-2 receptors angiotensin-converting enzyme 2 and transmembrane serine protease 2 was noted.
Conclusions and relevance: In this cohort study, there was no evidence of placental infection or definitive vertical transmission of SARS-CoV-2. Transplacental transfer of anti-SARS-CoV-2 antibodies was inefficient. Lack of viremia and reduced coexpression and colocalization of placental angiotensin-converting enzyme 2 and transmembrane serine protease 2 may serve as protective mechanisms against vertical transmission.
Conflict of interest statement
Figures
Comment in
-
Protecting Pregnant Women and Their Infants From COVID-19: Clues From Maternal Viral Loads, Antibody Responses, and Placentas.JAMA Netw Open. 2020 Dec 1;3(12):e2030564. doi: 10.1001/jamanetworkopen.2020.30564. JAMA Netw Open. 2020. PMID: 33351080 No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
