

Long-Term Cause-Specific Mortality in Hodgkin Lymphoma Patients
- PMID: 33351090
- PMCID: PMC8168246
- DOI: 10.1093/jnci/djaa194
Long-Term Cause-Specific Mortality in Hodgkin Lymphoma Patients
Abstract
Background: Few studies have examined the impact of treatment-related morbidity on long-term, cause-specific mortality in Hodgkin lymphoma (HL) patients.
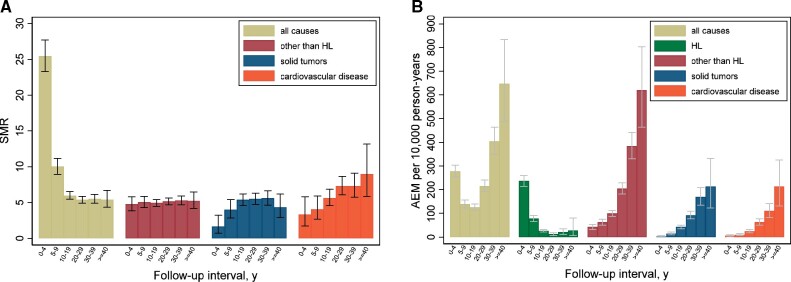
Methods: This multicenter cohort included 4919 HL patients, treated before age 51 years between 1965 and 2000, with a median follow-up of 20.2 years. Standardized mortality ratios, absolute excess mortality (AEM) per 10 000 person-years, and cause-specific cumulative mortality by stage and primary treatment, accounting for competing risks, were calculated.
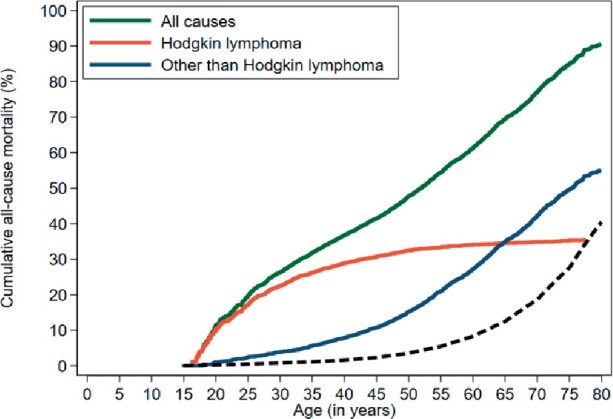
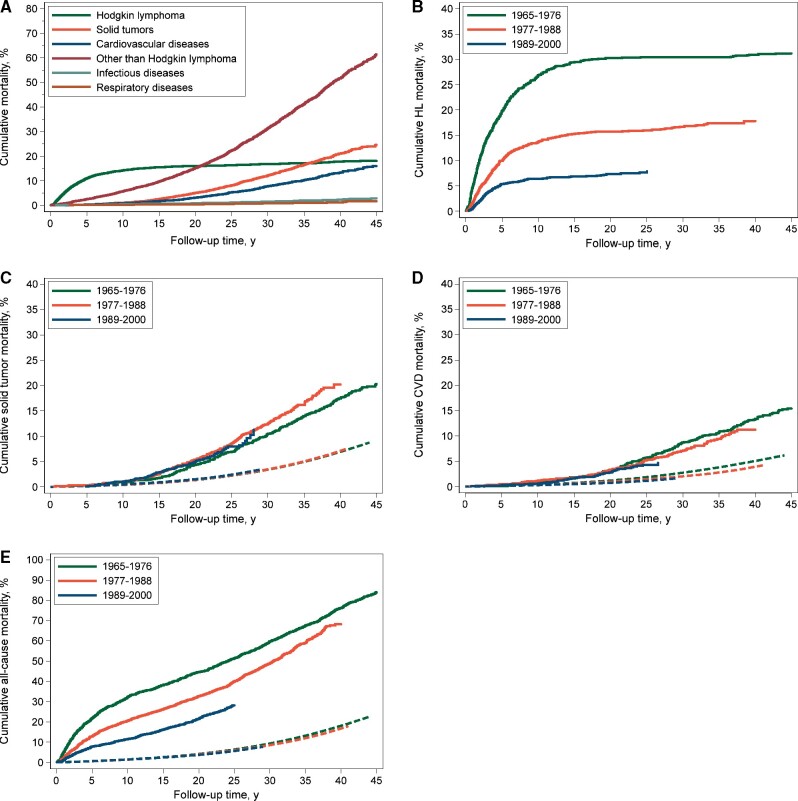
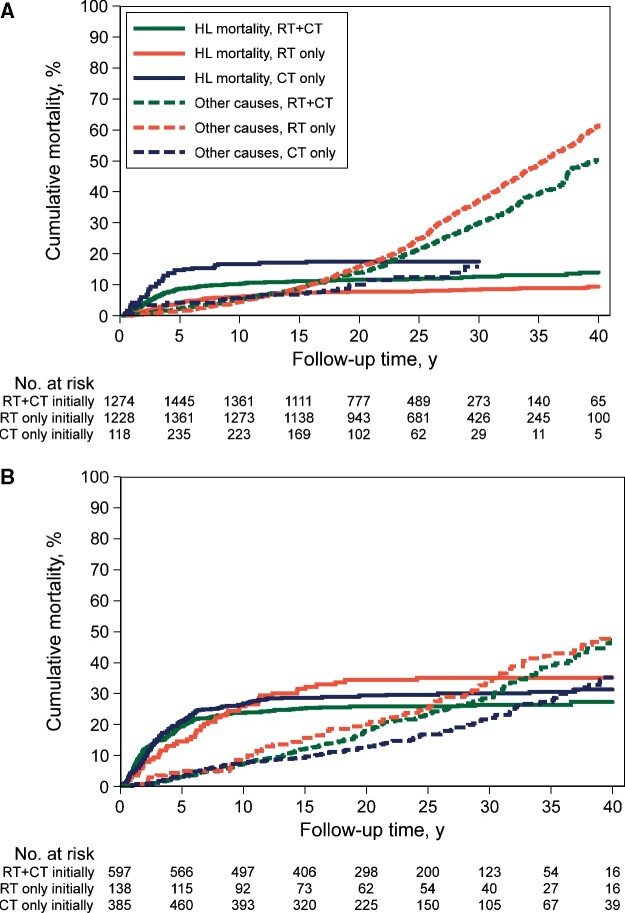
Results: HL patients experienced a 5.1-fold (AEM = 123 excess deaths per 10 000 person-years) higher risk of death due to causes other than HL. This risk remained increased in 40-year survivors (standardized mortality ratio = 5.2, 95% confidence interval [CI] = 4.2 to 6.5, AEM = 619). At age 54 years, HL survivors experienced similar cumulative mortality (20.0%) from causes other than HL to 71-year-old individuals from the general population. Whereas HL mortality statistically significantly decreased over the calendar period (P < .001), solid tumor mortality did not change in the most recent treatment era. Patients treated in 1989-2000 had lower 25-year cardiovascular disease mortality than patients treated in 1965-1976 (4.3% vs 5.7%; subdistribution hazard ratio = 0.65, 95% CI = 0.46 to 0.93). Infectious disease mortality was not only increased after splenectomy but also after spleen irradiation (hazard ratio = 2.81, 95% CI = 1.55 to 5.07). For stage I-II, primary treatment with chemotherapy (CT) alone was associated with statistically significantly higher HL mortality (P < .001 for CT vs radiotherapy [RT]; P = .04 for CT vs RT+CT) but lower 30-year mortality from causes other than HL (15.8%, 95% CI = 9.7% to 23.3%) compared with RT alone (36.9%, 95% CI = 34.0% to 39.8%, P = .001) and RT and CT combined (29.8%, 95% CI = 26.8% to 32.9%, P = .02).
Conclusions: Compared with the general population, HL survivors have a substantially reduced life expectancy. Optimal selection of patients for primary CT is crucial, weighing risks of HL relapse and long-term toxicity.
© The Author(s) 2020. Published by Oxford University Press.
Figures
References
-
- Borchmann P, Eichenauer DA, Engert A. State of the art in the treatment of Hodgkin lymphoma. Nat Rev Clin Oncol. 2012;9(8):450–459. - PubMed
-
- van Leeuwen FE, Klokman WJ, Veer MB, et al. Long-term risk of second malignancy in survivors of Hodgkin's disease treated during adolescence or young adulthood. J Clin Oncol. 2000;18(3):487–497. - PubMed
-
- Ng AK, Bernardo MV, Weller E, et al. Second malignancy after Hodgkin disease treated with radiation therapy with or without chemotherapy: long-term risks and risk factors. Blood. 2002;100(6):1989–1996. - PubMed
-
- Swerdlow AJ, Higgins CD, Smith P, et al. Second cancer risk after chemotherapy for Hodgkin's lymphoma: a collaborative British cohort study. J Clin Oncol. 2011;29(31):4096–4104. - PubMed
-
- Schaapveld M, Aleman BM, van Eggermond AM, et al. Second cancer risk up to 40 years after treatment for Hodgkin's lymphoma. N Engl J Med. 2015;373(26):2499–2511. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
