

Erythrocytosis in the general population: clinical characteristics and association with clonal hematopoiesis
- PMID: 33351130
- PMCID: PMC7757002
- DOI: 10.1182/bloodadvances.2020003323
Erythrocytosis in the general population: clinical characteristics and association with clonal hematopoiesis
Abstract
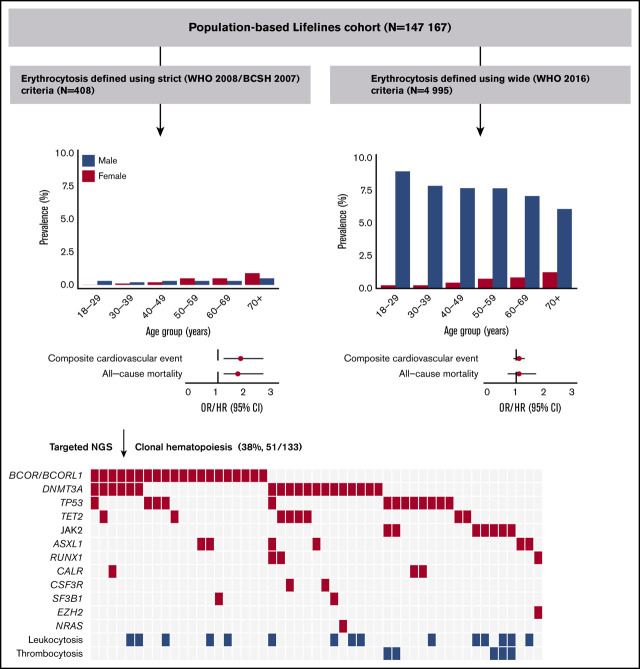
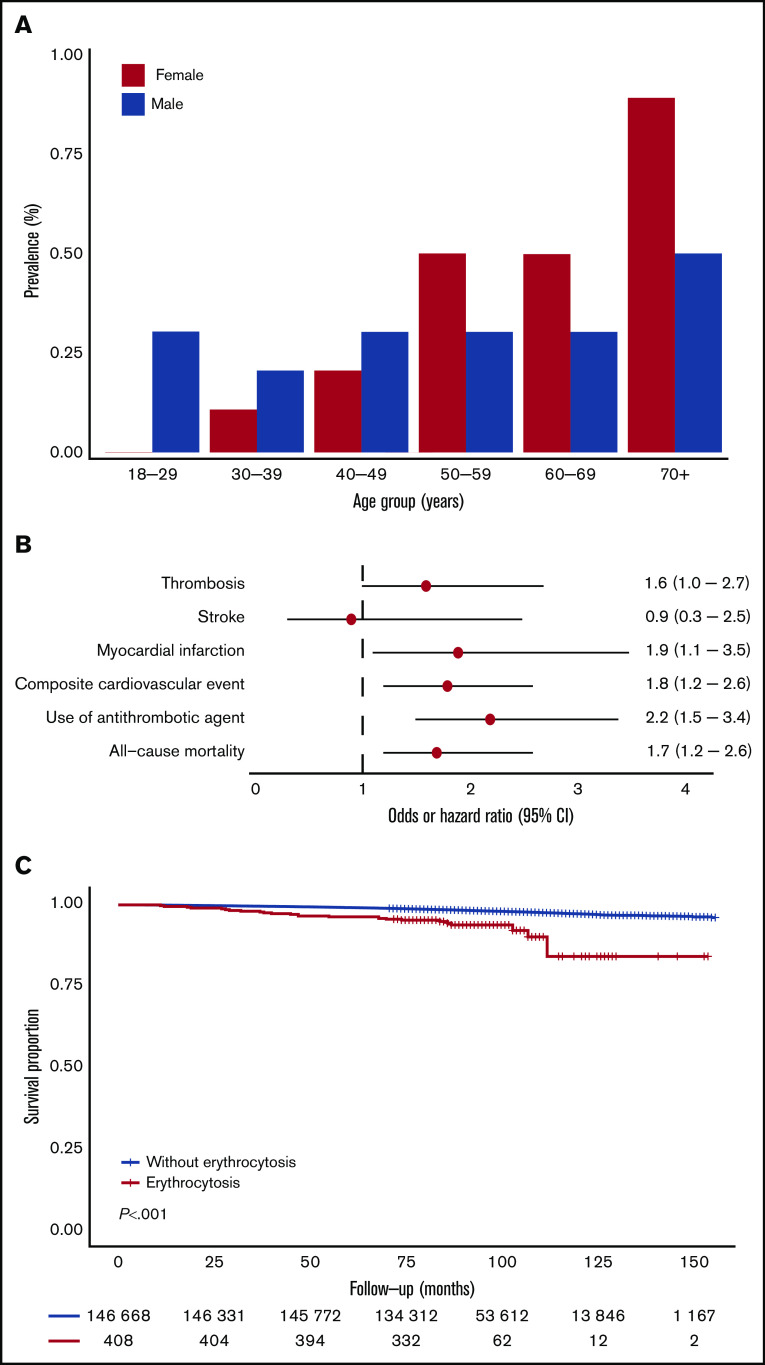
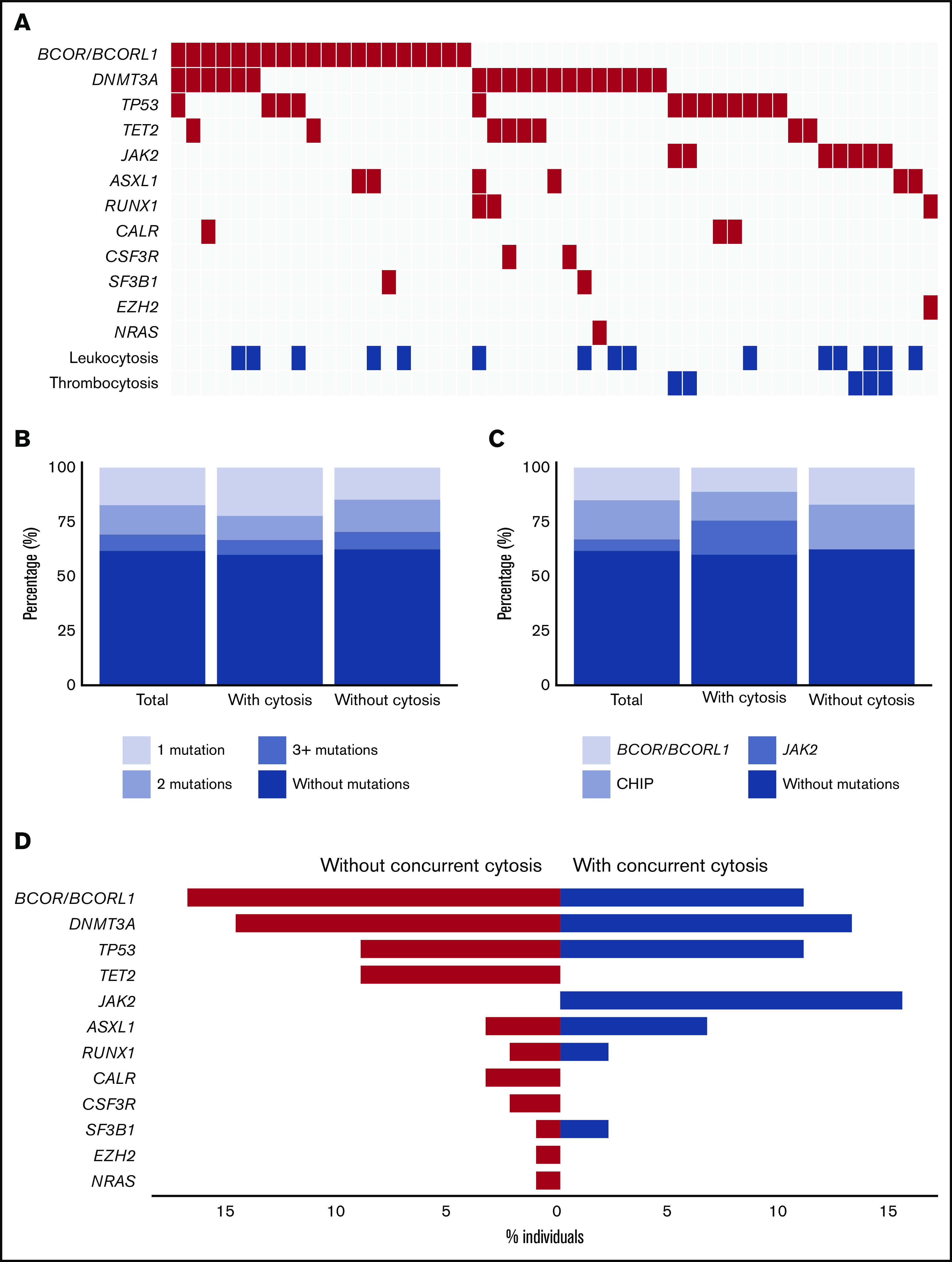
Erythrocytosis is a common reason for referral to hematology services and is usually secondary in origin. The aim of this study was to assess clinical characteristics and clonal hematopoiesis (CH) in individuals with erythrocytosis in the population-based Lifelines cohort (n = 147 167). Erythrocytosis was defined using strict (World Health Organization [WHO] 2008/British Committee for Standards in Hematology) and wide (WHO 2016) criteria. Individuals with erythrocytosis (strict criteria) and concurrent leukocytosis and/or thrombocytosis were 1:2 matched with individuals with isolated erythrocytosis and analyzed for somatic mutations indicative of CH (≥5% variant allele frequency). One hundred eighty five males (0.3%) and 223 females (0.3%) met the strict criteria, whereas 4868 males (7.6%) and 309 females (0.4%) met the wide criteria. Erythrocytosis, only when defined using strict criteria, was associated with cardiovascular morbidity (odds ratio [OR], 1.8; 95% confidence interval [CI], 1.2-2.6), cardiovascular mortality (hazard ratio [HR], 2.2; 95% CI, 1.0-4.6), and all-cause mortality (HR, 1.7; 95% CI, 1.2-2.6), independent of conventional risk factors. Mutations were detected in 51 of 133 (38%) evaluable individuals, with comparable frequencies between individuals with and without concurrent cytosis. The JAK2 V617F mutation was observed in 7 of 133 (5.3%) individuals, all having concurrent cytosis. The prevalence of mutations in BCOR/BCORL1 (16%) was high, suggesting aberrant epigenetic regulation. Erythrocytosis with CH was associated with cardiovascular morbidity (OR, 9.1; 95% CI, 1.2-68.4) in a multivariable model. Our data indicate that only when defined using strict criteria erythrocytosis is associated with cardiovascular morbidity (especially in the presence of CH), cardiovascular mortality, and all-cause mortality.
© 2020 by The American Society of Hematology.
Conflict of interest statement
Conflict-of-interest disclosure: The authors declare no competing financial interests.
Figures
References
-
- McMullin MF. The classification and diagnosis of erythrocytosis. Int J Lab Hematol. 2008;30(6):447-459. - PubMed
-
- Mehta J, Wang H, Iqbal SU, Mesa R. Epidemiology of myeloproliferative neoplasms in the United States. Leuk Lymphoma. 2014;55(3):595-600. - PubMed
-
- Passamonti F, Rumi E, Pungolino E, et al. Life expectancy and prognostic factors for survival in patients with polycythemia vera and essential thrombocythemia. Am J Med. 2004;117(10):755-761. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
