

Risk factors for severity of COVID-19 in chronic dialysis patients from a multicentre French cohort
- PMID: 33354330
- PMCID: PMC7743188
- DOI: 10.1093/ckj/sfaa199
Risk factors for severity of COVID-19 in chronic dialysis patients from a multicentre French cohort
Abstract
Background: Coronavirus disease 2019 (COVID-19) is an emerging infectious disease, related to severe acute respiratory syndrome coronavirus 2 infection. Few data are available in patients with end-stage renal disease (ESRD).
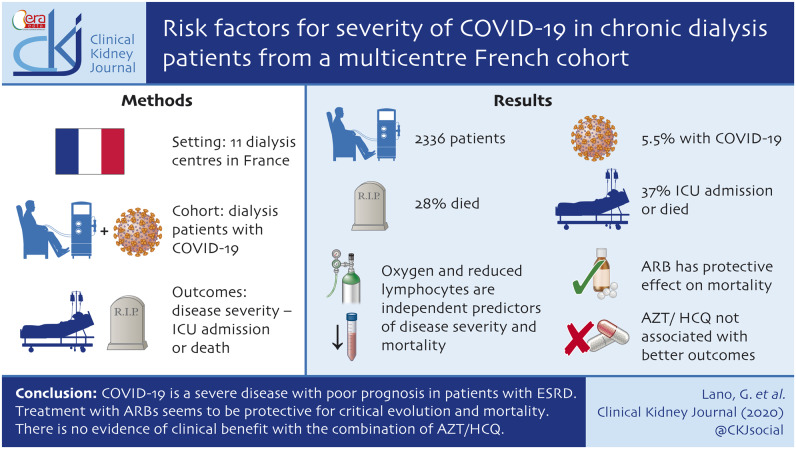
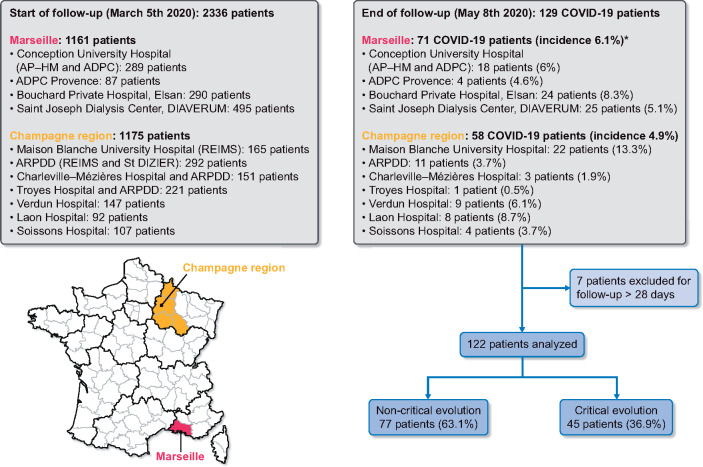
Methods: We conducted an observational cohort study of COVID-19 patients at 11 dialysis centres in two distinct districts of France to examine the epidemiological and clinical characteristics of COVID-19 in this population, and to determine risk factors of disease severity (defined as a composite outcome including intensive care unit admission or death) and mortality.
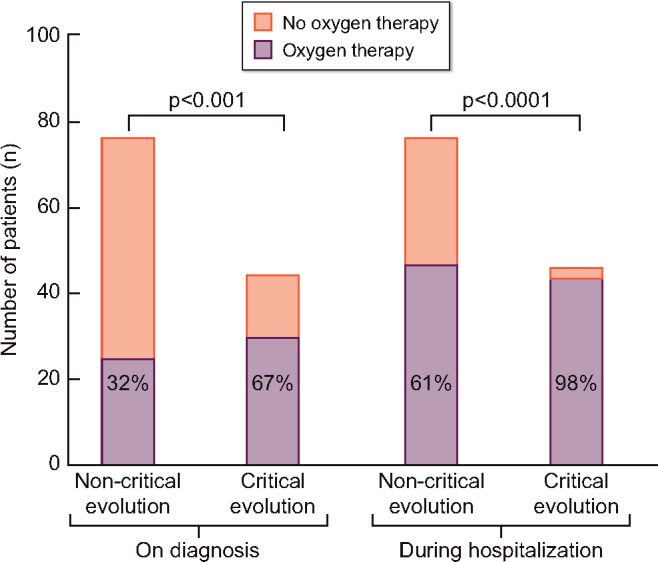
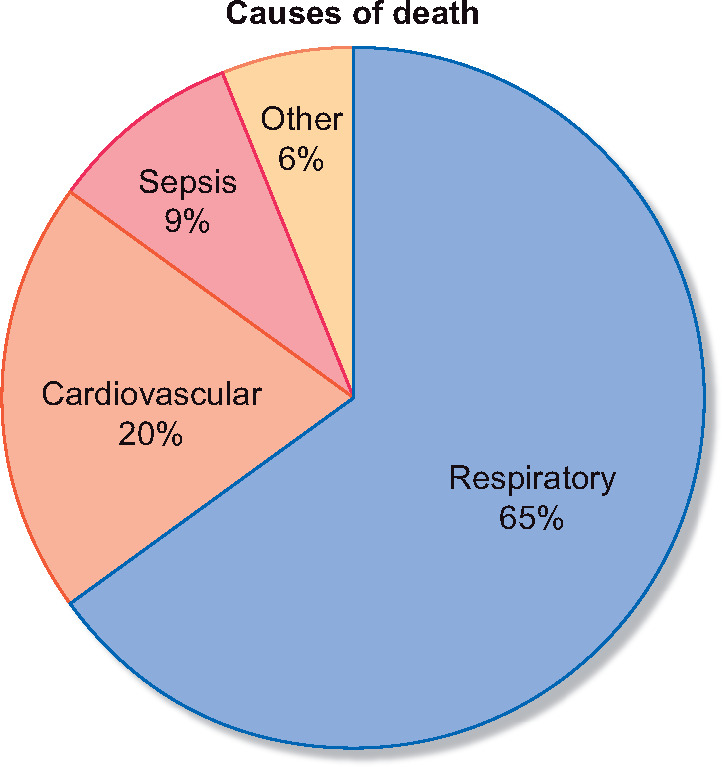
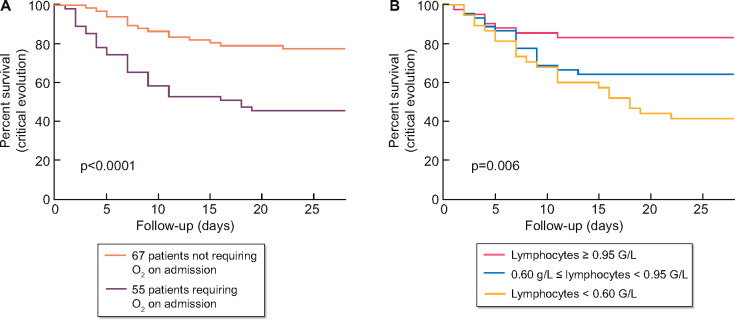
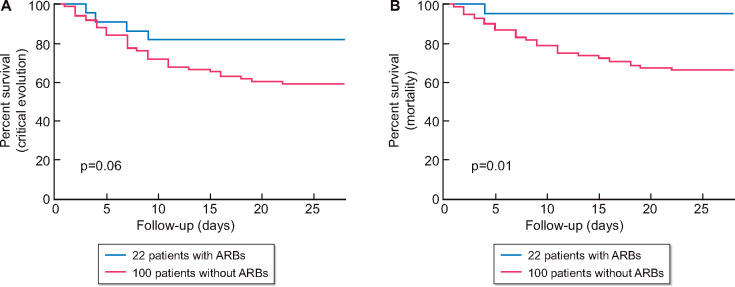
Results: Among the 2336 patients enrolled, 5.5% had confirmed COVID-19 diagnosis. Of the 122 patients with a follow-up superior to 28 days, 37% reached the composite outcome and 28% died. Multivariate analysis showed that oxygen therapy on diagnosis and a decrease in lymphocyte count were independent risk factors associated with disease severity and with mortality. Chronic use of angiotensin II receptor blockers (ARBs) (18% of patients) was associated with a protective effect on mortality. Treatment with azithromycin and hydroxychloroquine (AZT/HCQ) (46% of patients) were not associated with the composite outcome and with death in univariate and multivariate analyses.
Conclusions: COVID-19 is a severe disease with poor prognosis in patients with ESRD. Usual treatment with ARBs seems to be protective of critical evolution and mortality. There is no evidence of clinical benefit with the combination of AZT/HCQ.
Keywords: COVID-19; angiotensin II receptor blockers; dialysis; hydroxychloroquine; lymphocytes.
© The Author(s) 2020. Published by Oxford University Press on behalf of ERA-EDTA.
Figures
Comment on
-
Complement and protection from tissue injury in COVID-19.Clin Kidney J. 2020 Oct 4;13(5):734-738. doi: 10.1093/ckj/sfaa196. eCollection 2020 Oct. Clin Kidney J. 2020. PMID: 33123353 Free PMC article.
References
-
- Wiersinga WJ, Rhodes A, Cheng AC. et al. Pathophysiology, transmission, diagnosis, and treatment of coronavirus disease 2019 (COVID-19): a review. JAMA 2020; 324: 782. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
