

Atelectrauma Versus Volutrauma: A Tale of Two Time-Constants
- PMID: 33354673
- PMCID: PMC7746208
- DOI: 10.1097/CCE.0000000000000299
Atelectrauma Versus Volutrauma: A Tale of Two Time-Constants
Abstract
Objectives: Elucidate how the degree of ventilator-induced lung injury due to atelectrauma that is produced in the injured lung during mechanical ventilation is determined by both the timing and magnitude of the airway pressure profile.
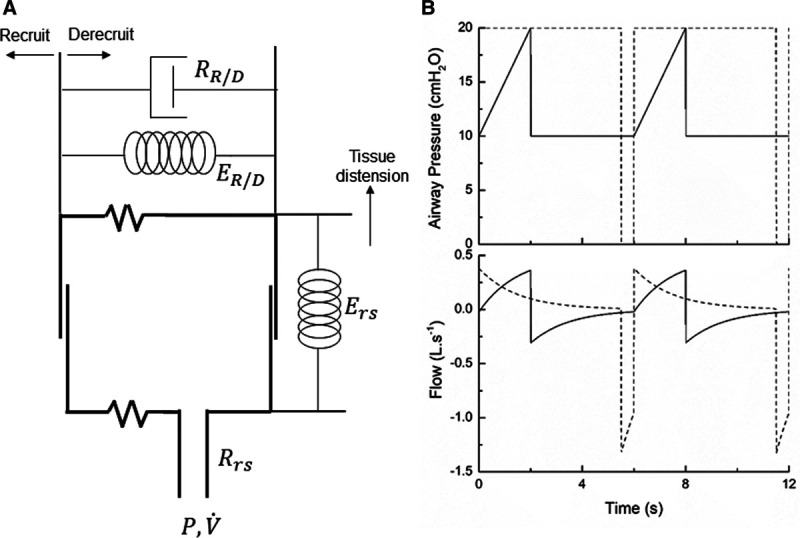
Design: A computational model of the injured lung provides a platform for exploring how mechanical ventilation parameters potentially modulate atelectrauma and volutrauma. This model incorporates the time dependence of lung recruitment and derecruitment, and the time-constant of lung emptying during expiration as determined by overall compliance and resistance of the respiratory system.
Setting: Computational model.
Subjects: Simulated scenarios representing patients with both normal and acutely injured lungs.
Measurements and main results: Protective low-tidal volume ventilation (Low-Vt) of the simulated injured lung avoided atelectrauma through the elevation of positive end-expiratory pressure while maintaining fixed tidal volume and driving pressure. In contrast, airway pressure release ventilation avoided atelectrauma by incorporating a very brief expiratory duration () that both prevents enough time for derecruitment and limits the minimum alveolar pressure prior to inspiration. Model simulations demonstrated that has an effective threshold value below which airway pressure release ventilation is safe from atelectrauma while maintaining a tidal volume and driving pressure comparable with those of Low-Vt. This threshold is strongly influenced by the time-constant of lung-emptying.
Conclusions: Low-Vt and airway pressure release ventilation represent markedly different strategies for the avoidance of ventilator-induced lung injury, primarily involving the manipulation of positive end-expiratory pressure and , respectively. can be based on exhalation flow values, which may provide a patient-specific approach to protective ventilation.
Keywords: acute respiratory distress syndrome; computational model; lung elastance; mechanical ventilation; recruitment and derecruitment; ventilator-induced lung injury; volutrauma.
Copyright © 2020 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of the Society of Critical Care Medicine.
Conflict of interest statement
Dr. Bates is a consultant for and shareholder in Oscillavent and LLC (Iowa), and a coapplicant on the patent “Variable ventilation as a diagnostic tool for assessing lung mechanical function” PCT Application WO2015127377 A1, Filed on February 23, 2014 (C538); Mr. Nieman has an Unrestricted Educational Grant from Dräger Medical; Dr. Habashi is founder of Intensive Care On-line Network, lectured at symposia sponsored in part by an unrestricted educational grant from Dräger Medical, holds patents that have not been commercialized, licensed or produced royalties on a method of initiating, managing and/or weaning airway pressure release ventilation, and controlling a ventilator in accordance with the same. Dr. Gaver has disclosed that he does not have any potential conflicts of interest.
Figures
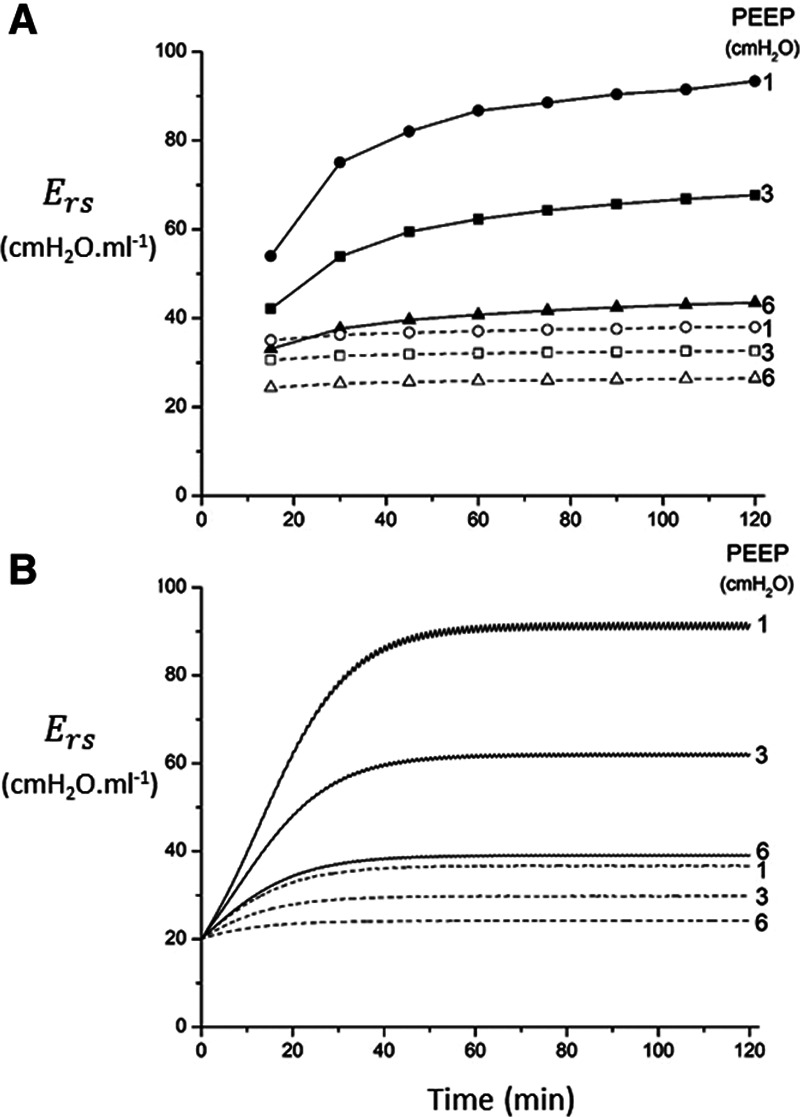

 ), driving pressure (Pdriving), and tidal volume as a function of positive end-expiratory pressure (PEEP) for Low-V
), driving pressure (Pdriving), and tidal volume as a function of positive end-expiratory pressure (PEEP) for Low-V = 10 s and (B)
= 10 s and (B)  = 2 s. Peak airway pressure was 10 cm H2O above PEEP in all cases. Dashed lines: healthy lung; solid lines: injured lung. Note that
= 2 s. Peak airway pressure was 10 cm H2O above PEEP in all cases. Dashed lines: healthy lung; solid lines: injured lung. Note that  remains relatively high until PEEP reaches approximately 15 cm H2O.
remains relatively high until PEEP reaches approximately 15 cm H2O.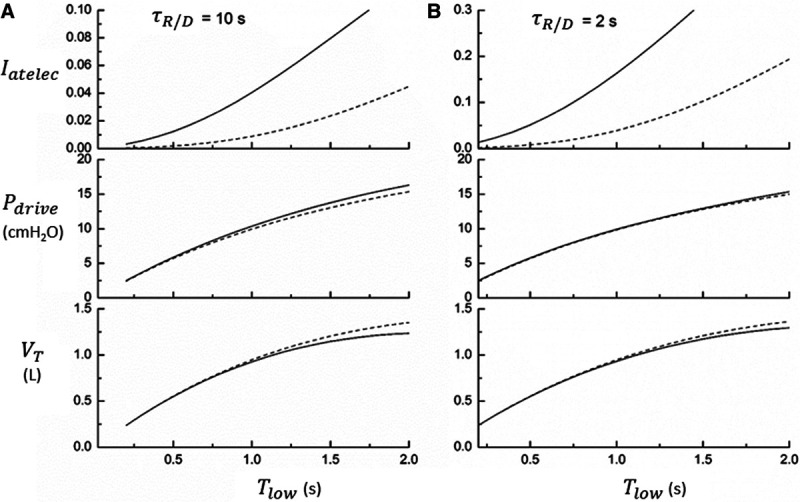
 ), driving pressure (Pdriving), and tidal volume as a function of
), driving pressure (Pdriving), and tidal volume as a function of  for low-V
for low-V = 10 s and (B)
= 10 s and (B)  = 2 s. Peak airway pressure was 10 cm H2O above positive end-expiratory pressure in all cases. Dashed lines: healthy lung; solid lines: injured lung. Note that
= 2 s. Peak airway pressure was 10 cm H2O above positive end-expiratory pressure in all cases. Dashed lines: healthy lung; solid lines: injured lung. Note that  is low until
is low until  reaches approximately 0.5 s, after which it rises dramatically as
reaches approximately 0.5 s, after which it rises dramatically as  is further increased.
is further increased.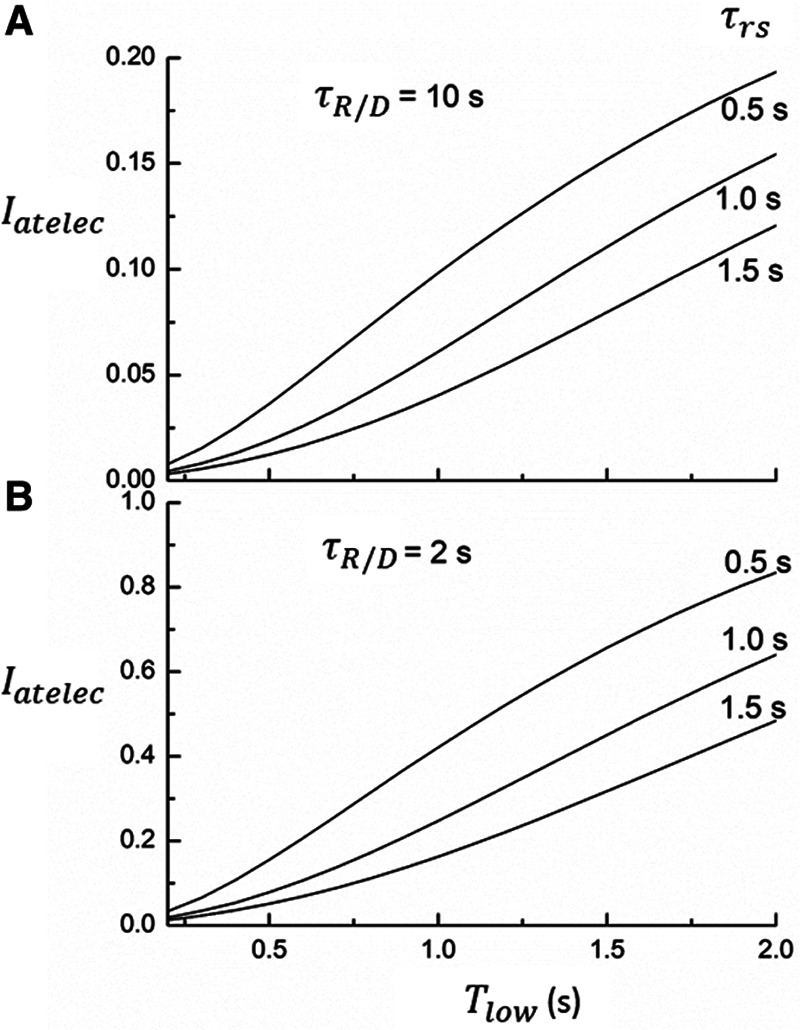
 ) as a function of
) as a function of  during ventilation of the injured lung with airway pressure release ventilation for (A)
during ventilation of the injured lung with airway pressure release ventilation for (A)  = 10 s and (B)
= 10 s and (B)  = 2 s, showing the effects of reducing the time-constant of emptying of the lung achieved by varying airway resistance (Raw).
= 2 s, showing the effects of reducing the time-constant of emptying of the lung achieved by varying airway resistance (Raw).References
-
- Ferguson ND, Cook DJ, Guyatt GH, et al. ; OSCILLATE Trial Investigators; Canadian Critical Care Trials Group. High-frequency oscillation in early acute respiratory distress syndrome. N Engl J Med. 2013; 368:795–805 - PubMed
-
- Young D, Lamb SE, Shah S, et al. ; OSCAR Study Group. High-frequency oscillation for acute respiratory distress syndrome. N Engl J Med. 2013; 368:806–813 - PubMed
-
- Cavalcanti AB, Suzumura ÉA, Laranjeira LN, et al. ; Writing Group for the Alveolar Recruitment for Acute Respiratory Distress Syndrome Trial (ART) Investigators. Effect of lung recruitment and titrated positive end-expiratory pressure (PEEP) vs low PEEP on mortality in patients with acute respiratory distress syndrome: A randomized clinical trial. JAMA. 2017; 318:1335–1345 - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
