

Association Between ICU-Acquired Hypernatremia and In-Hospital Mortality: Data From the Medical Information Mart for Intensive Care III and the Electronic ICU Collaborative Research Database
- PMID: 33354677
- PMCID: PMC7746205
- DOI: 10.1097/CCE.0000000000000304
Association Between ICU-Acquired Hypernatremia and In-Hospital Mortality: Data From the Medical Information Mart for Intensive Care III and the Electronic ICU Collaborative Research Database
Abstract
Objectives: Describe the relationship between ICU-acquired hypernatremia and in-hospital mortality and investigate the optimal hypernatremia correction rate.
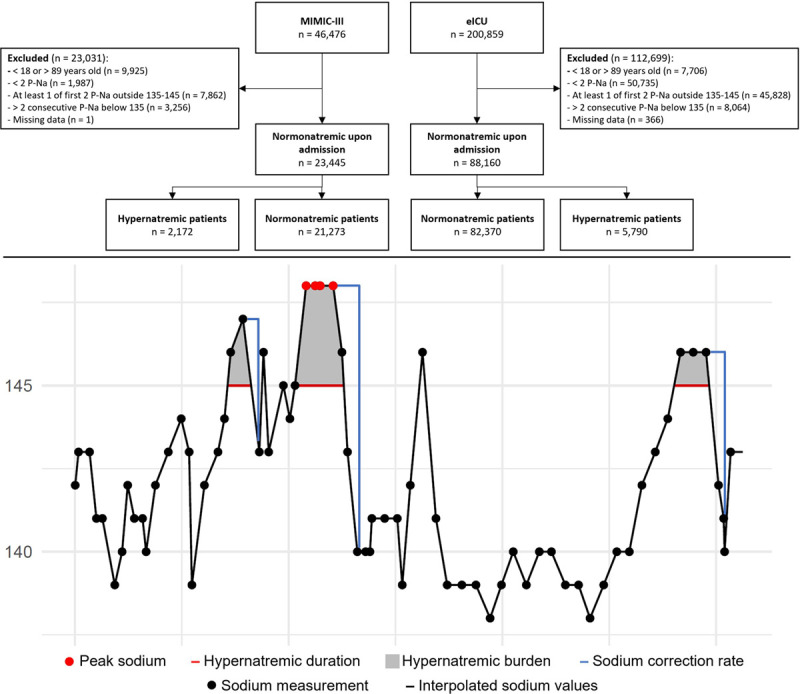
Design setting participants and measurements: Observational study including two individual ICU cohorts. We used the Medical Information Mart for Intensive Care III v. 1.4 database consists of all ICU patients admitted to the Beth Israel Deaconess Medical Center in Boston from 2001 to 2012 (n = 46,476). The electronic ICU v. 2.0 database consists of all ICU patients admitted to 208 distinct hospitals across the United States from 2014 to 2015 (n = 200,859). We included all adult patients admitted to an ICU with two consecutive sodium samples within normal range (135-145 mmol/L) and without two consecutive hyponatremic samples (< 135 mmol/L) during the ICU stay.
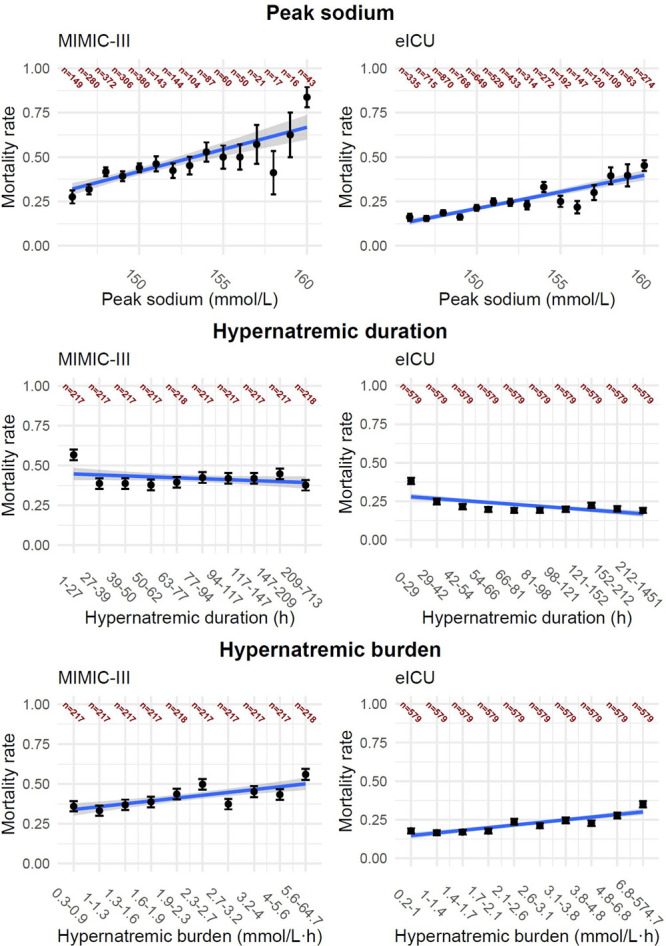
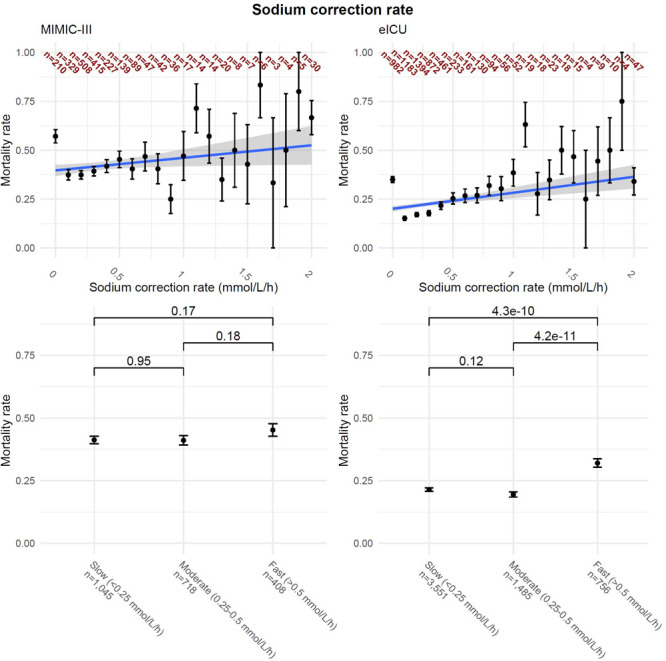
Results: Of 23,445 patients identified in Medical Information Mart for Intensive Care III, 9% (n = 2,172) developed hypernatremia during their ICU stay. In electronic ICU, 88,160 patients were identified and 7% (n = 5,790) developed hypernatremia. In both cohorts, patients with hypernatremia had a higher mortality (Medical Information Mart for Intensive Care III: 20% vs 42%; p < 0.01 and electronic ICU: 6% vs 22%; p < 0.01), with hypernatremia increasing the risk of in-hospital mortality (Medical Information Mart for Intensive Care III: odds ratio, 1.15; 95% CI, 1.13-1.17 and electronic ICU: odds ratio, 1.11; 95% CI, 1.10-1.12) and over time using a Cox regression. Rapid sodium correction rate (> 0.5 mmol/L/hr) was associated with an increased in-hospital mortality in both cohorts (Medical Information Mart for Intensive Care III: odds ratio, 1.08; 95% CI, 1.03-1.13 and electronic ICU: odds ratio, 1.10; 95% CI, 1.06-1.13). In the electronic ICU cohort, rapid correction rates were associated with a significant difference in in-hospital mortality, but there was no statistically significant association in the Medical Information Mart for Intensive Care III cohort.
Conclusions: ICU-acquired hypernatremia is associated with increased in-hospital mortality. Furthermore, a rapid sodium correction rates may be harmful. This suggests it is important to both prevent ICU-acquired hypernatremia and to avoid rapid correction rates if a patient becomes hypernatremic.
Keywords: Medical Information Mart for Intensive Care III; correction rates; electronic ICU Collaborative Research Database; hypernatremia; mortality.
Copyright © 2020 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of the Society of Critical Care Medicine.
Conflict of interest statement
Dr. Sherak received funding from the Albert Einstein Office of Medical Student Research to travel to the Datathon. The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
References
-
- Lindner G, Funk G-C. Hypernatremia in critically ill patients. J Crit Care. 2013; 28:216.e11–e20 - PubMed
-
- Sarahian S, Pouria MM, Ing TS, et al. Hypervolemic hypernatremia is the most common type of hypernatremia in the intensive care unit. Int Urol Nephrol. 2015; 47:1817–1821 - PubMed
-
- Sterns RH. Hypernatremia in the intensive care unit: Instant quality–just add water. Crit Care Med. 1999; 27:1041–1042 - PubMed
LinkOut - more resources
Full Text Sources
