

DNA Polymerase and Mismatch Repair Exert Distinct Microsatellite Instability Signatures in Normal and Malignant Human Cells
- PMID: 33355208
- PMCID: PMC8223607
- DOI: 10.1158/2159-8290.CD-20-0790
DNA Polymerase and Mismatch Repair Exert Distinct Microsatellite Instability Signatures in Normal and Malignant Human Cells
Abstract
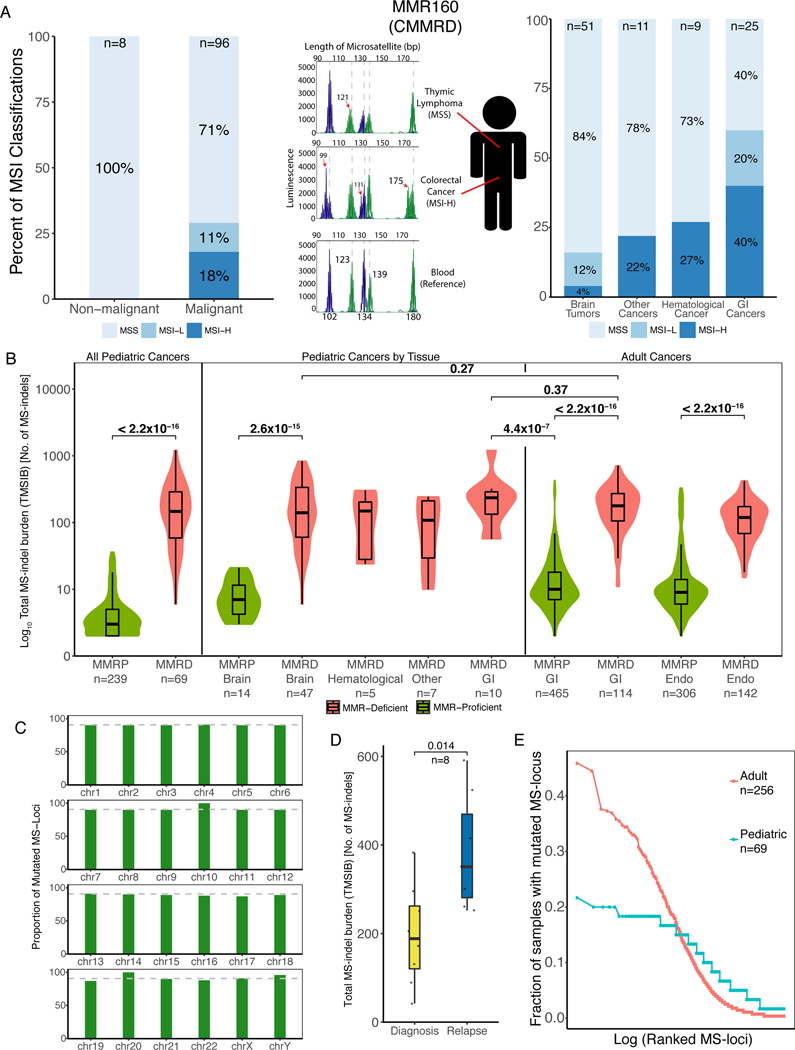
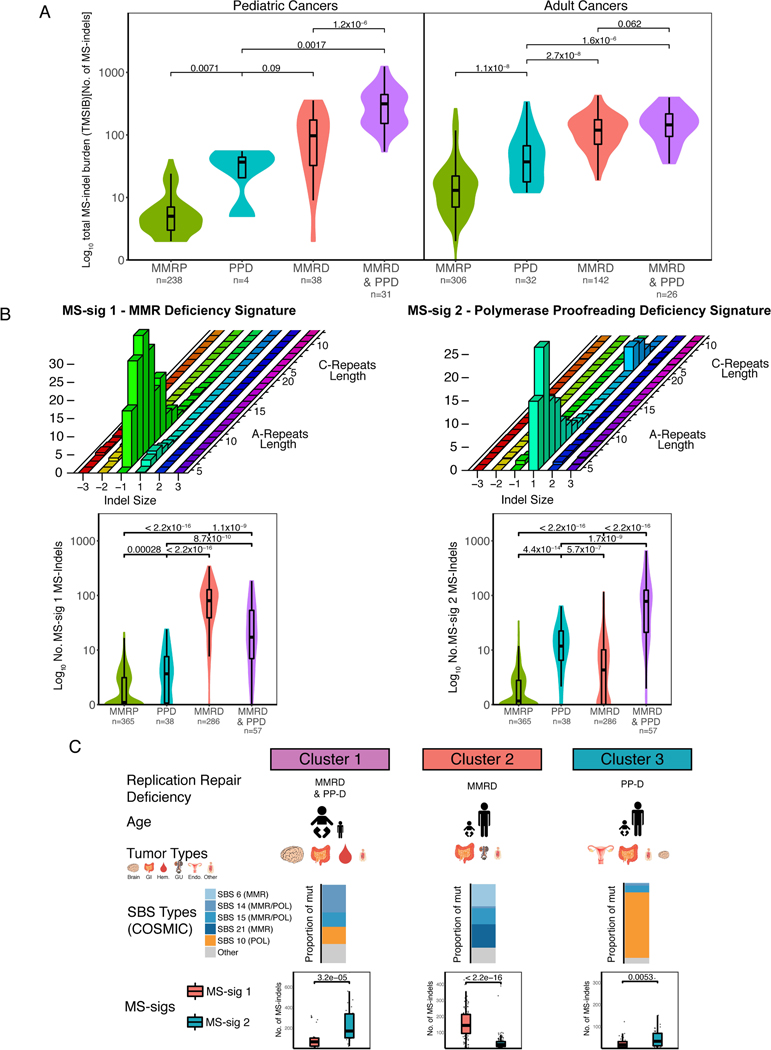
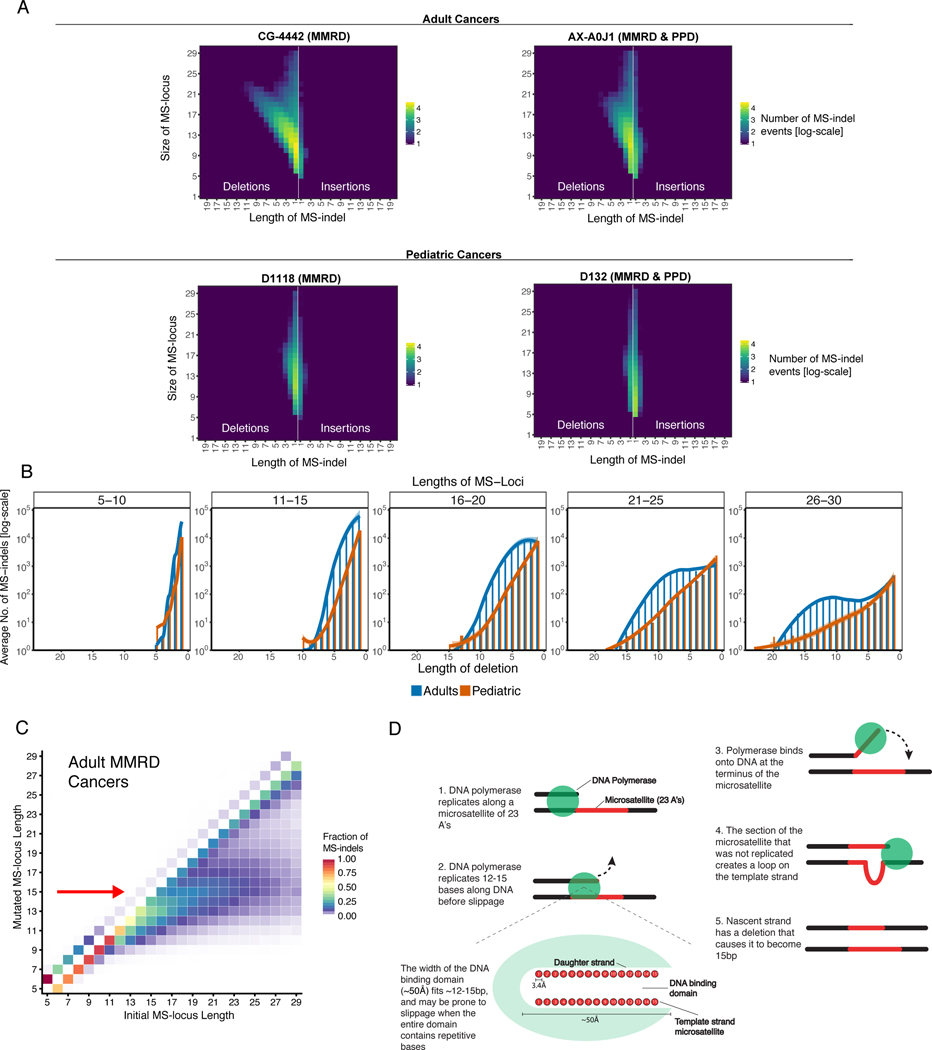
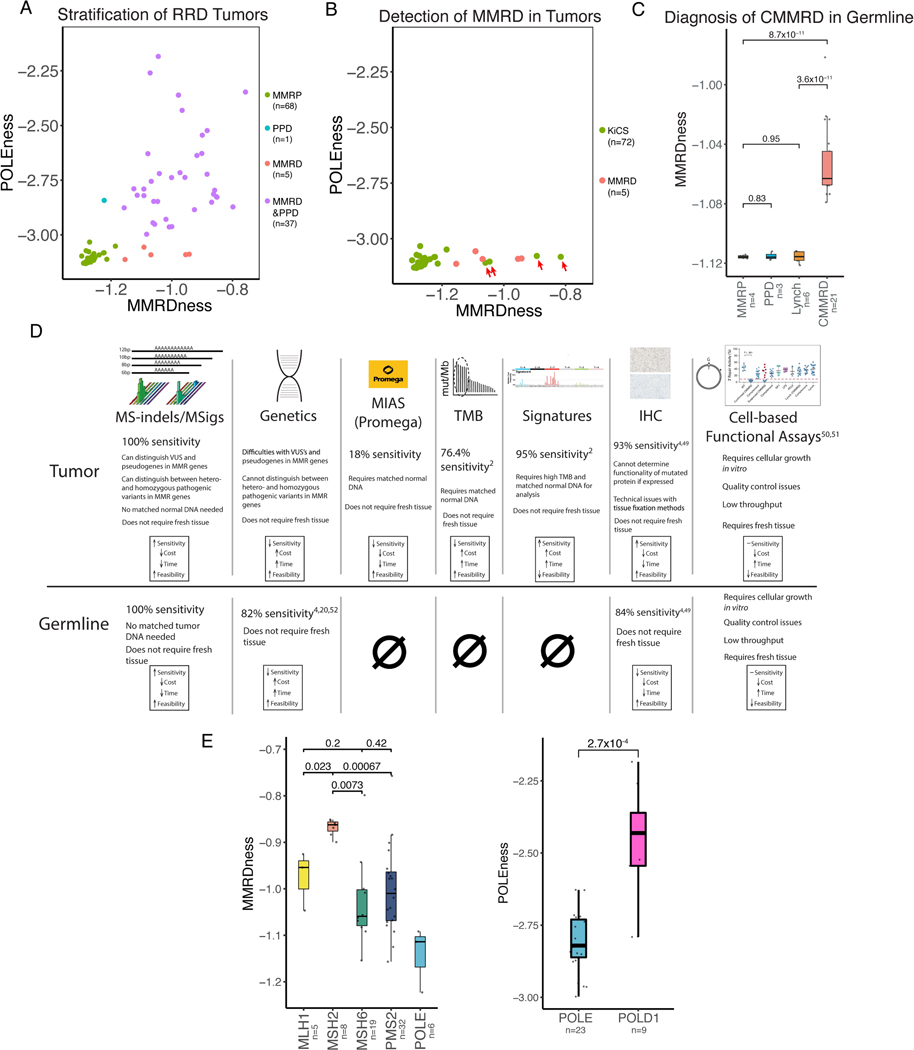
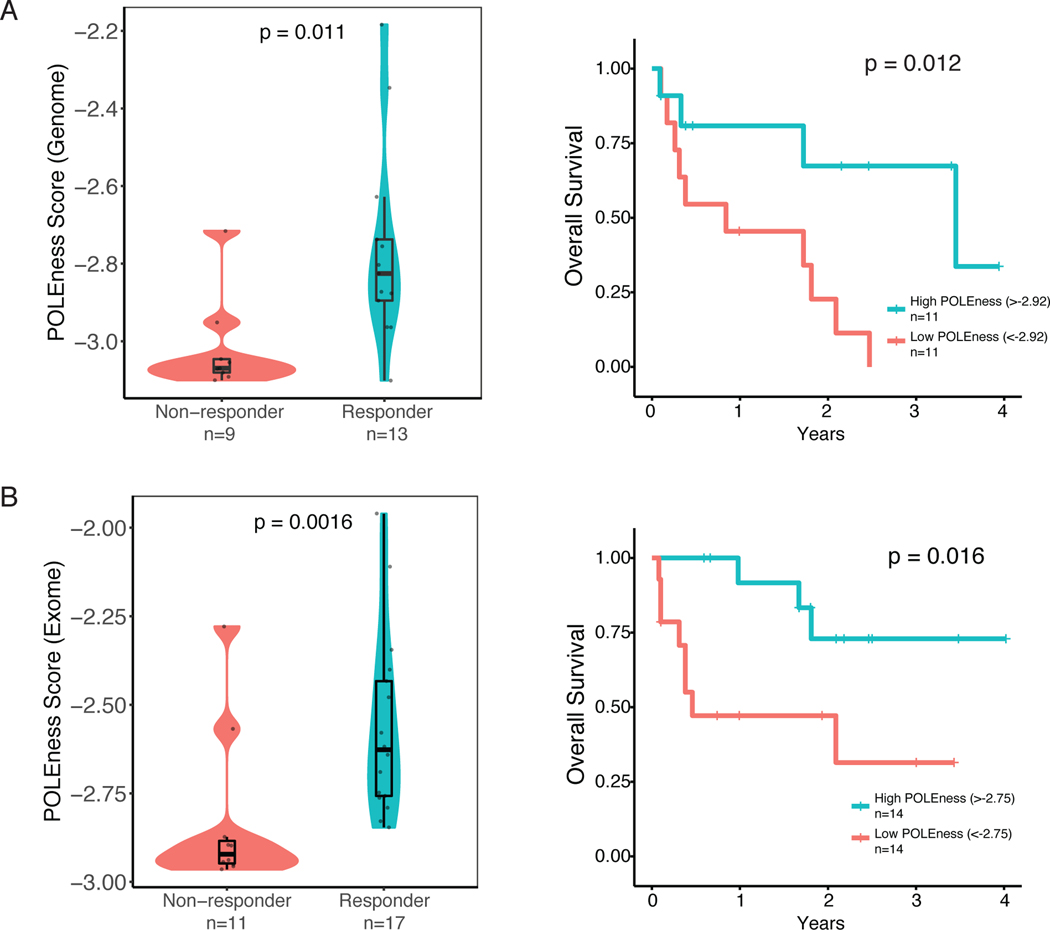
Although replication repair deficiency, either by mismatch repair deficiency (MMRD) and/or loss of DNA polymerase proofreading, can cause hypermutation in cancer, microsatellite instability (MSI) is considered a hallmark of MMRD alone. By genome-wide analysis of tumors with germline and somatic deficiencies in replication repair, we reveal a novel association between loss of polymerase proofreading and MSI, especially when both components are lost. Analysis of indels in microsatellites (MS-indels) identified five distinct signatures (MS-sigs). MMRD MS-sigs are dominated by multibase losses, whereas mutant-polymerase MS-sigs contain primarily single-base gains. MS deletions in MMRD tumors depend on the original size of the MS and converge to a preferred length, providing mechanistic insight. Finally, we demonstrate that MS-sigs can be a powerful clinical tool for managing individuals with germline MMRD and replication repair-deficient cancers, as they can detect the replication repair deficiency in normal cells and predict their response to immunotherapy. SIGNIFICANCE: Exome- and genome-wide MSI analysis reveals novel signatures that are uniquely attributed to mismatch repair and DNA polymerase. This provides new mechanistic insight into MS maintenance and can be applied clinically for diagnosis of replication repair deficiency and immunotherapy response prediction.This article is highlighted in the In This Issue feature, p. 995.
©2020 American Association for Cancer Research.
Conflict of interest statement
Conflicts of Interest:
G.G. is a founder, consultant and holds privately held equity in Scorpion Therapeutics. G.G. receives research funds from IBM and Pharmacyclics. G.G. is an inventor on patent applications related to MuTect, ABSOLUTE, MutSig and POLYSOLVER. Y.E.M and G.G. are inventors on patent applications related to MSMuTect and MSMutSig. G.G., Y.E.M., U.T., and J.C. are inventors on patent applications related to MSIdetect. Other authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
