

Advanced Liver Fibrosis Is Common in Patients With Type 2 Diabetes Followed in the Outpatient Setting: The Need for Systematic Screening
- PMID: 33355256
- PMCID: PMC7818321
- DOI: 10.2337/dc20-1997
Advanced Liver Fibrosis Is Common in Patients With Type 2 Diabetes Followed in the Outpatient Setting: The Need for Systematic Screening
Abstract
Objective: Assess the prevalence of nonalcoholic fatty liver disease (NAFLD) and of liver fibrosis associated with nonalcoholic steatohepatitis in unselected patients with type 2 diabetes mellitus (T2DM).
Research design and methods: A total of 561 patients with T2DM (age: 60 ± 11 years; BMI: 33.4 ± 6.2 kg/m2; and HbA1c: 7.5 ± 1.8%) attending primary care or endocrinology outpatient clinics and unaware of having NAFLD were recruited. At the visit, volunteers were invited to be screened by elastography for steatosis and fibrosis by controlled attenuation parameter (≥274 dB/m) and liver stiffness measurement (LSM; ≥7.0 kPa), respectively. Secondary causes of liver disease were ruled out. Diagnostic panels for prediction of advanced fibrosis, such as AST-to-platelet ratio index (APRI) and Fibrosis-4 (FIB-4) index, were also measured. A liver biopsy was performed if results were suggestive of fibrosis.
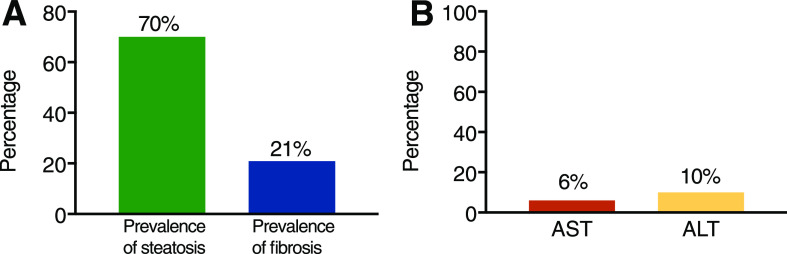
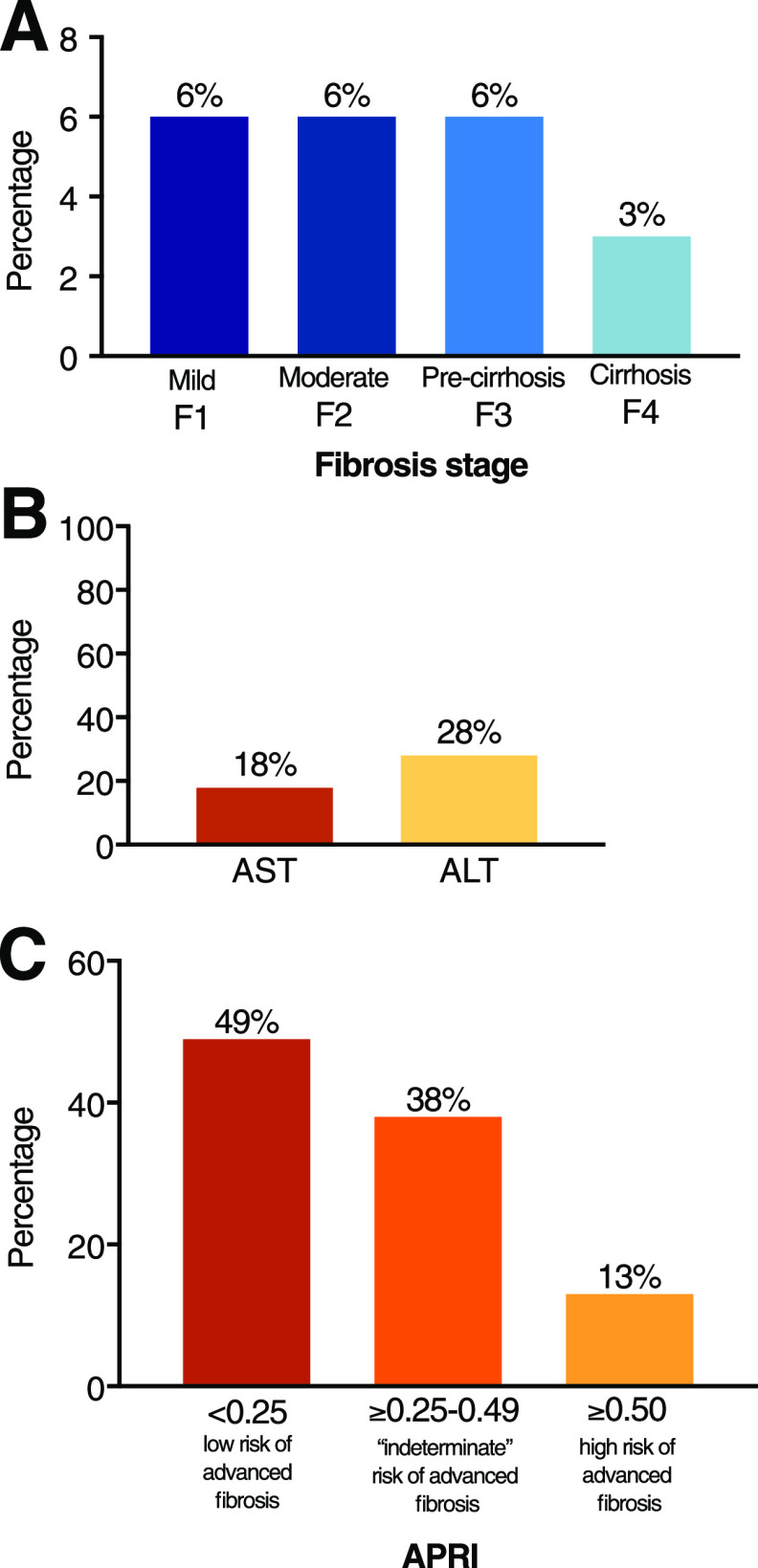
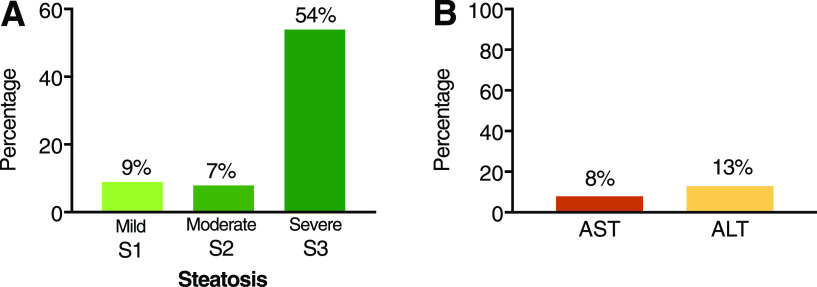
Results: The prevalence of steatosis was 70% and of fibrosis 21% (LSM ≥7.0 kPa). Moderate fibrosis (F2: LSM ≥8.2 kPa) was present in 6% and severe fibrosis or cirrhosis (F3-4: LSM ≥9.7 kPa) in 9%, similar to that estimated by FIB-4 and APRI panels. Noninvasive testing was consistent with liver biopsy results. Elevated AST or ALT ≥40 units/L was present in a minority of patients with steatosis (8% and 13%, respectively) or with liver fibrosis (18% and 28%, respectively). This suggests that AST/ALT alone are insufficient as initial screening. However, performance may be enhanced by imaging (e.g., transient elastography) and plasma diagnostic panels (e.g., FIB-4 and APRI).
Conclusions: Moderate-to-advanced fibrosis (F2 or higher), an established risk factor for cirrhosis and overall mortality, affects at least one out of six (15%) patients with T2DM. These results support the American Diabetes Association guidelines to screen for clinically significant fibrosis in patients with T2DM with steatosis or elevated ALT.
© 2020 by the American Diabetes Association.
Figures
References
-
- Budd J, Cusi K. Nonalcoholic fatty liver disease: what does the primary care physician need to know? Am J Med 2020;133:536–543 - PubMed
-
- Younossi ZM, Golabi P, de Avila L, et al. The global epidemiology of NAFLD and NASH in patients with type 2 diabetes: a systematic review and meta-analysis. J Hepatol 2019;71:793–801 - PubMed
-
- Chalasani N, Younossi Z, Lavine JE, et al. The diagnosis and management of nonalcoholic fatty liver disease: practice guidance from the American Association for the Study of Liver Diseases. Hepatology 2018;67:328–357 - PubMed
-
- European Association for the Study of the Liver; European Association for the Study of Diabetes; European Association for the Study of Obesity EASL-EASD-EASO clinical practice guidelines for the management of non-alcoholic fatty liver disease. Diabetologia 2016;59:1121–1140 - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
