

Comparative effectiveness and safety of direct oral anticoagulants versus vitamin K antagonists in nonvalvular atrial fibrillation: a Canadian multicentre observational cohort study
- PMID: 33355273
- PMCID: PMC7759115
- DOI: 10.9778/cmajo.20200055
Comparative effectiveness and safety of direct oral anticoagulants versus vitamin K antagonists in nonvalvular atrial fibrillation: a Canadian multicentre observational cohort study
Abstract
Background: Direct oral anticoagulants (DOACs) have widely replaced warfarin for stroke prevention in nonvalvular atrial fibrillation. Our objective was to compare the safety and effectiveness of DOACs (dabigatran, rivaroxaban, apixaban) versus warfarin for stroke prevention in nonvalvular atrial fibrillation in the Canadian setting.
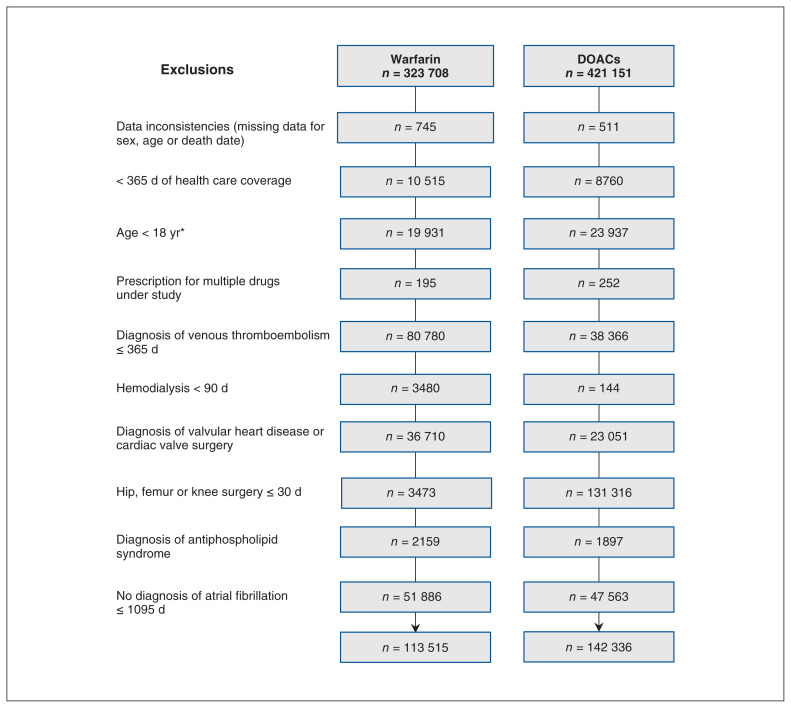
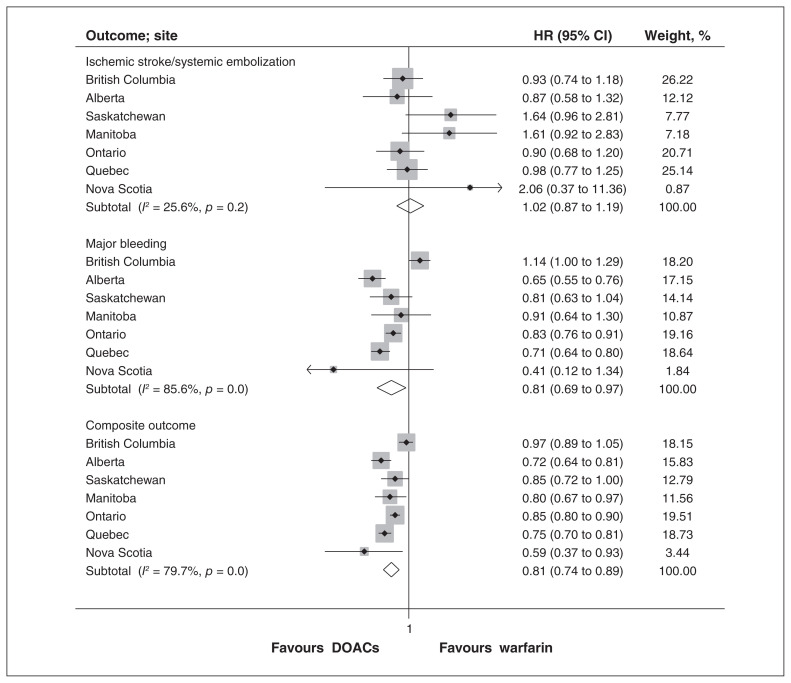
Methods: We conducted a population-based observational multicentre cohort study with propensity score matching and subsequent meta-analysis. We used health care databases from 7 Canadian provinces (British Columbia, Alberta, Saskatchewan, Manitoba, Ontario, Quebec and Nova Scotia). Patients with nonvalvular atrial fibrillation who initiated anticoagulation therapy in 2009-2017 were matched to an equal number who initiated warfarin. The primary outcome was the pooled hazard ratio (HR) for ischemic stroke or systemic embolization. Secondary outcomes included pooled HRs for major bleeding; a composite outcome of stroke, systemic embolization, major bleeding and all-cause mortality; and myocardial infarction. We modelled HRs using proportional hazard Cox regression with inverse probability of censoring weights, and estimated pooled HRs with random-effect meta-analyses.
Results: We included 128 273 patients who initiated anticoagulation with a DOAC (40 503 dabigatran, 49 498 rivaroxaban and 38 272 apixaban) and 128 273 patients who initiated anticoagulation with warfarin. The pooled HR for ischemic stroke or systemic embolization comparing DOACs to warfarin was 1.02 (95% confidence interval [CI] 0.87 to 1.19). Direct oral anticoagulants were associated with lower rates of major bleeding (pooled HR 0.81, 95% CI 0.69 to 0.97), the composite outcome (pooled HR 0.81, 95% CI 0.74 to 0.89) and all-cause mortality (pooled HR 0.81, 95% CI 0.78 to 0.85).
Interpretation: In this real-world study, DOACs were associated with similar risks of ischemic stroke or systemic embolization, and lower risks of bleeding and total mortality compared to warfarin. These findings support the use of DOACs for anticoagulation in nonvalvular atrial fibrillation.
Trial registration: ClinicalTrials.gov, no. NCT03596502.
Copyright 2020, Joule Inc. or its licensors.
Conflict of interest statement
Competing interests: Min Jun has received unrestricted grant support from VentureWise, a wholly owned subsidiary of NPS MedicineWise funded by AstraZeneca. No other competing interests were declared.
Figures
References
-
- Atrial fibrillation. Ottawa: Heart and Stroke Foundation; [accessed 2020 Dec. 10]. Available: www.heartandstroke.ca/heart-disease/conditions/atrial-fibrillation.
-
- Verma A, Cairns JA, Mitchell LB, et al. CCS Atrial Fibrillation Guidelines Committee. 2014 focused update of the Canadian Cardiovascular Society Guidelines for the management of atrial fibrillation. Can J Cardiol. 2014;30:1114–30. - PubMed
-
- National Clinical Guideline Centre (UK) Atrial fibrillation: the management of atrial fibrillation. London (UK): National Institute for Health and Care Excellence; 2014. - PubMed
-
- January CT, Wann LS, Calkins H, et al. 2019 AHA/ACC/HRS focused update of the 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation. Circulation. 2019;140:e125–51. - PubMed
-
- Andrade JG, Verma A, Mitchell LB, et al. 2018 focused update of the Canadian Cardiovascular Society guidelines for the management of atrial fibrillation. Can J Cardiol. 2018;34:1371–92. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical