

COVID-19 screening of asymptomatic patients admitted through emergency departments in Alberta: a prospective quality-improvement study
- PMID: 33355274
- PMCID: PMC7759116
- DOI: 10.9778/cmajo.20200191
COVID-19 screening of asymptomatic patients admitted through emergency departments in Alberta: a prospective quality-improvement study
Abstract
Background: The prevalence of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection among asymptomatic patients admitted to hospital has implications for personal protective equipment use, testing strategy and confidence in the safety of acute care services. Our aim was to estimate the positivity rate of reverse transcription polymerase chain reaction (RT-PCR) testing among people admitted to hospital without symptoms of coronavirus disease 2019 (COVID-19) in Alberta, Canada.
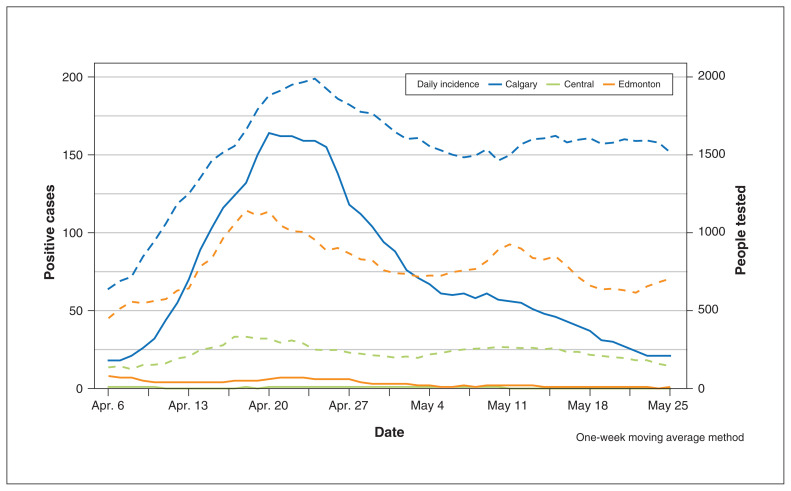
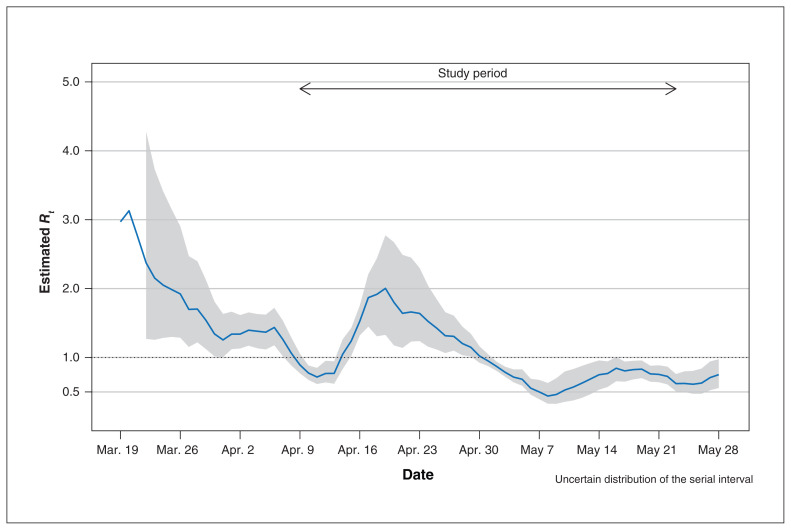
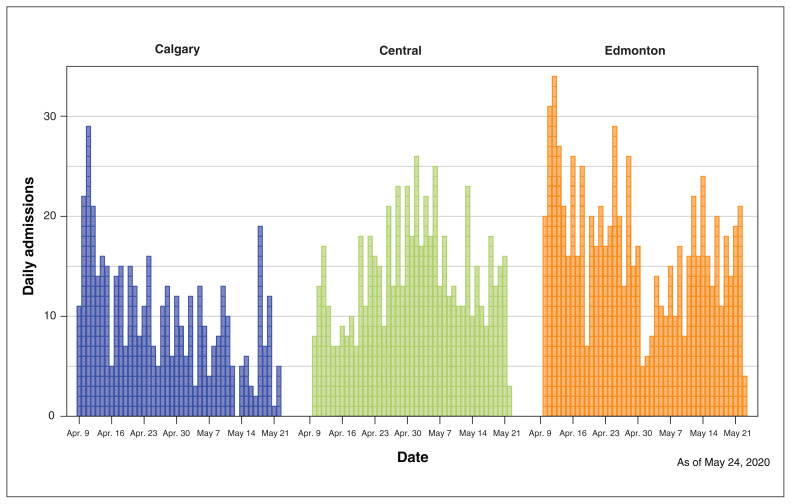
Methods: Between Apr. 9 and May 24, 2020, we screened for COVID-19 symptoms and tested for SARS-CoV-2 infection in all consecutive adult patients (≥ 18 yr) admitted via emergency department to 3 Alberta hospitals. We summarized the parameters of the epidemic curve and assessed the performance of symptom screening versus RT-PCR results on nasopharyngeal or oropharyngeal swab samples.
Results: The study period encompassed Alberta's initial epidemic curve, with peak active cases per 100 000 of 71.4 (0.07%) on Apr. 30, 2020, and 14.7 and 14.6 at the beginning (Apr. 9, 2020) and end (May 24, 2020), respectively. Testing for SARS-CoV-2 infection (64.9% throat and 35.1% nasopharyngeal swabs) was done on 3375 adults (mean age 51, standard deviation 21, yr; 51.5% men). None of the asymptomatic patients (n = 1814) tested positive, and 71 of those with symptoms tested positive (n = 1561; 4.5%, 95% confidence interval [CI] 3.6%-5.7%). Sensitivity of symptom screening (v. RT-PCR) was 100% (95% CI 95%-100%), and specificity was 55% (95% CI 53%-57%). Posttest probabilities for prevalence of SARS-CoV-2 infection ranging from 1.5 to 14 times the peak prevalence of active cases during the study did not change when we assumed lower sensitivity (92%).
Interpretation: In a region with low disease prevalence where protocolized symptom assessment was in place during the admission process, we did not identify people admitted to hospital without COVID-19 symptoms who were RT-PCR positive. There may not be additive benefit to universal testing of asymptomatic patients on hospital admission in a setting of low pretest probability and strong public health containment.
Copyright 2020, Joule Inc. or its licensors.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Coronavirus disease (COVID-19): How is it transmitted? Geneva: World Health Organization; 2020. [accessed 2020 Dec. 4]. Available: www.who.int/news-room/q-a-detail/coronavirus-disease-covid-19-how-is-it-....
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous