

Laparoscopic Lavage vs Primary Resection for Acute Perforated Diverticulitis: Long-term Outcomes From the Scandinavian Diverticulitis (SCANDIV) Randomized Clinical Trial
- PMID: 33355658
- PMCID: PMC7758831
- DOI: 10.1001/jamasurg.2020.5618
Laparoscopic Lavage vs Primary Resection for Acute Perforated Diverticulitis: Long-term Outcomes From the Scandinavian Diverticulitis (SCANDIV) Randomized Clinical Trial
Erratum in
-
Error in Results and Table.JAMA Surg. 2021 Sep 1;156(9):894. doi: 10.1001/jamasurg.2021.3556. JAMA Surg. 2021. PMID: 34319371 Free PMC article. No abstract available.
Abstract
Importance: Perforated colonic diverticulitis usually requires surgical resection, with significant morbidity. Short-term results from randomized clinical trials have indicated that laparoscopic lavage is a feasible alternative to resection. However, it appears that no long-term results are available.
Objective: To compare long-term (5-year) outcomes of laparoscopic peritoneal lavage and primary resection as treatments of perforated purulent diverticulitis.
Design, setting, and participants: This international multicenter randomized clinical trial was conducted in 21 hospitals in Sweden and Norway, which enrolled patients between February 2010 and June 2014. Long-term follow-up was conducted between March 2018 and November 2019. Patients with symptoms of left-sided acute perforated diverticulitis, indicating urgent surgical need and computed tomography-verified free air, were eligible. Those available for trial intervention (Hinchey stages <IV) were included in the long-term follow-up.
Interventions: Patients were assigned to undergo laparoscopic peritoneal lavage or colon resection based on computer-generated, center-stratified block randomization.
Main outcomes and measures: The primary outcome was severe complications within 5 years. Secondary outcomes included mortality, secondary operations, recurrences, stomas, functional outcomes, and quality of life.
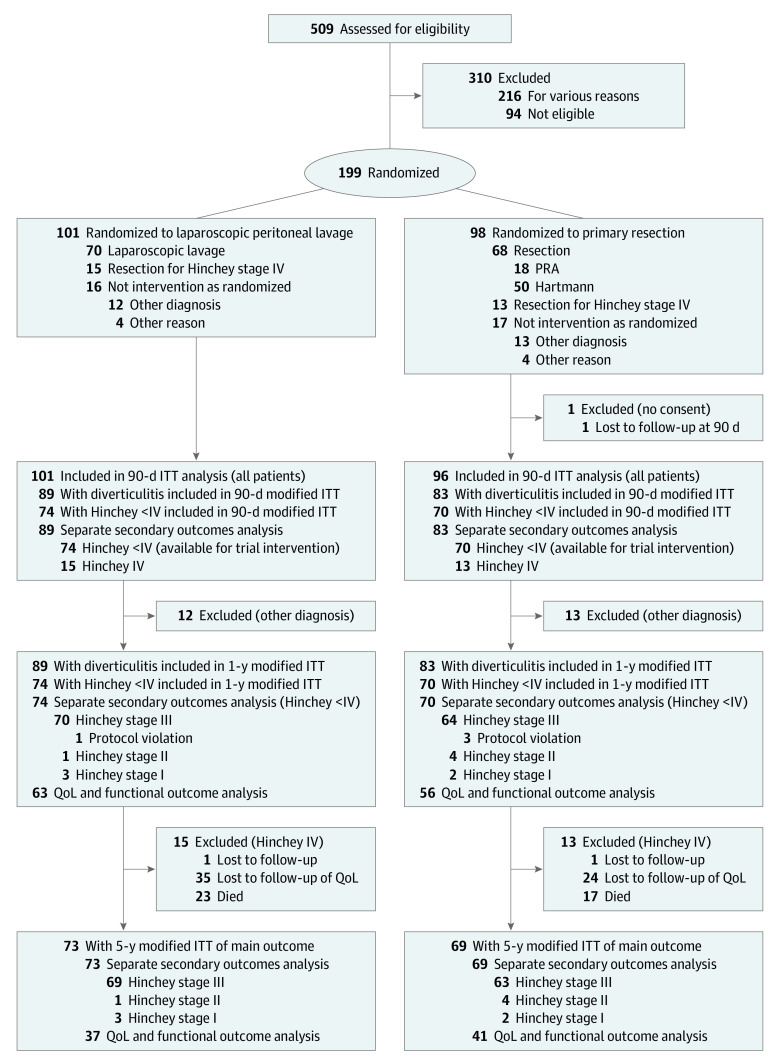
Results: Of 199 randomized patients, 101 were assigned to undergo laparoscopic peritoneal lavage and 98 were assigned to colon resection. At the time of surgery, perforated purulent diverticulitis was confirmed in 145 patients randomized to lavage (n = 74) and resection (n = 71). The median follow-up was 59 (interquartile range, 51-78; full range, 0-110) months, and 3 patients were lost to follow-up, leaving a final analysis of 73 patients who had had laparoscopic lavage (mean [SD] age, 66.4 [13] years; 39 men [53%]) and 69 who had received a resection (mean [SD] age, 63.5 [14] years; 36 men [52%]). Severe complications occurred in 36% (n = 26) in the laparoscopic lavage group and 35% (n = 24) in the resection group (P = .92). Overall mortality was 32% (n = 23) in the laparoscopic lavage group and 25% (n = 17) in the resection group (P = .36). The stoma prevalence was 8% (n = 4) in the laparoscopic lavage group vs 33% (n = 17; P = .002) in the resection group among patients who remained alive, and secondary operations, including stoma reversal, were performed in 36% (n = 26) vs 35% (n = 24; P = .92), respectively. Recurrence of diverticulitis was higher following laparoscopic lavage (21% [n = 15] vs 4% [n = 3]; P = .004). In the laparoscopic lavage group, 30% (n = 21) underwent a sigmoid resection. There were no significant differences in the EuroQoL-5D questionnaire or Cleveland Global Quality of Life scores between the groups.
Conclusions and relevance: Long-term follow-up showed no differences in severe complications. Recurrence of diverticulitis after laparoscopic lavage was more common, often leading to sigmoid resection. This must be weighed against the lower stoma prevalence in this group. Shared decision-making considering both short-term and long-term consequences is encouraged.
Trial registration: ClinicalTrials.gov Identifier: NCT01047462.
Conflict of interest statement
Figures
Comment in
-
Laparoscopic Lavage vs Resection for Purulent Diverticulitis: Equipoise or Optimistic Perseverance?JAMA Surg. 2021 Feb 1;156(2):128. doi: 10.1001/jamasurg.2020.5665. JAMA Surg. 2021. PMID: 33355631 No abstract available.
-
Long-term Outcomes of Laparoscopic Lavage for Perforated Diverticulitis Remain Unfavorable.JAMA Surg. 2021 Nov 1;156(11):1070-1071. doi: 10.1001/jamasurg.2021.3305. JAMA Surg. 2021. PMID: 34319375 No abstract available.
-
Long-term Outcomes of Laparoscopic Lavage for Perforated Diverticulitis Remain Unfavorable-Reply.JAMA Surg. 2021 Nov 1;156(11):1071. doi: 10.1001/jamasurg.2021.3306. JAMA Surg. 2021. PMID: 34319382 No abstract available.
References
-
- Delvaux M Diverticular disease of the colon in Europe: epidemiology, impact on citizen health and prevention. Aliment Pharmacol Ther. 2003;18(suppl 3):71-74. - PubMed
-
- Morris CR, Harvey IM, Stebbings WS, Hart AR. Incidence of perforated diverticulitis and risk factors for death in a UK population. Br J Surg. 2008;95(7):876-881. - PubMed
-
- Schultz JK, Yaqub S, Wallon C, et al. ; SCANDIV Study Group . Laparoscopic lavage vs primary resection for acute perforated diverticulitis: the SCANDIV randomized clinical trial. JAMA. 2015;314(13):1364-1375. - PubMed
-
- Myers E, Hurley M, O’Sullivan GC, Kavanagh D, Wilson I, Winter DC. Laparoscopic peritoneal lavage for generalized peritonitis due to perforated diverticulitis. Br J Surg. 2008;95(1):97-101. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
