

Assessment of Air Contamination by SARS-CoV-2 in Hospital Settings
- PMID: 33355679
- PMCID: PMC7758808
- DOI: 10.1001/jamanetworkopen.2020.33232
Assessment of Air Contamination by SARS-CoV-2 in Hospital Settings
Erratum in
-
Error in Figure.JAMA Netw Open. 2021 Jan 4;4(1):e2037904. doi: 10.1001/jamanetworkopen.2020.37904. JAMA Netw Open. 2021. PMID: 33496789 Free PMC article. No abstract available.
Abstract
Importance: Controversy remains regarding the transmission routes of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).
Objective: To review current evidence on air contamination with SARS-CoV-2 in hospital settings and the factors associated with contamination, including viral load and particle size.
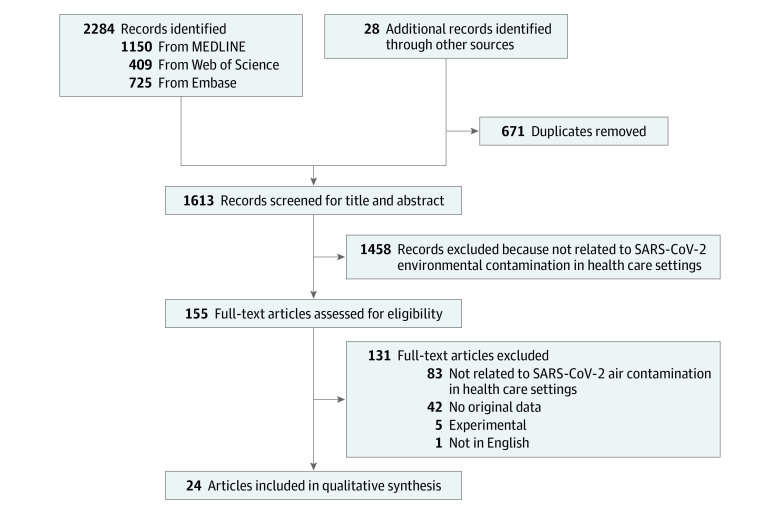
Evidence review: The MEDLINE, Embase, and Web of Science databases were systematically queried for original English-language articles detailing SARS-CoV-2 air contamination in hospital settings between January 1 and October 27, 2020. This study was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) guidelines. The positivity rate of SARS-CoV-2 viral RNA and culture were described and compared according to the setting, clinical context, air ventilation system, and distance from patients. The SARS-CoV-2 RNA concentrations in copies per meter cubed of air were pooled, and their distribution was described by hospital areas. Particle sizes and SARS-CoV-2 RNA concentrations in copies or median tissue culture infectious dose (TCID50) per meter cubed were analyzed after categorization as less than 1 μm, from 1 to 4 μm, and greater than 4 μm.
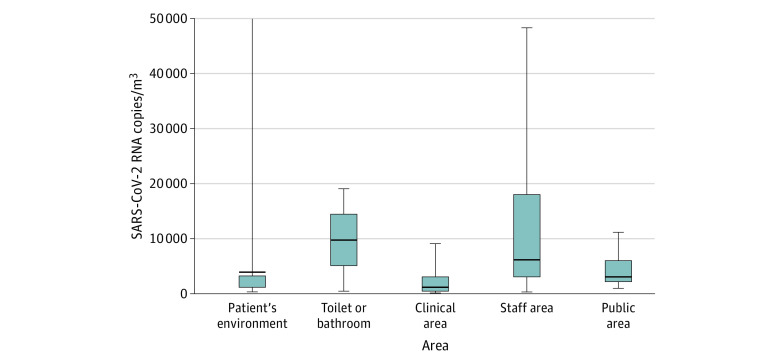
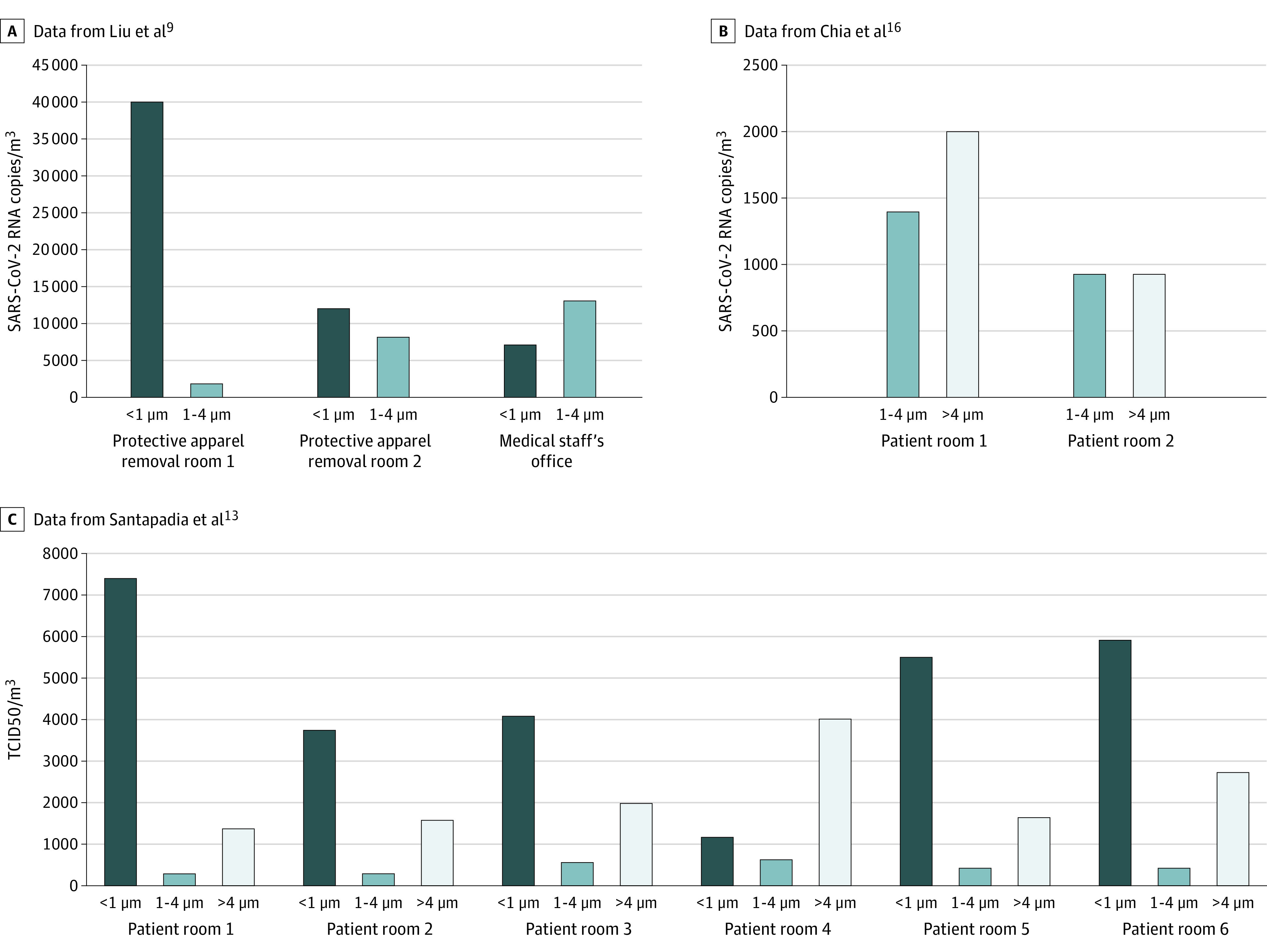
Findings: Among 2284 records identified, 24 cross-sectional observational studies were included in the review. Overall, 82 of 471 air samples (17.4%) from close patient environments were positive for SARS-CoV-2 RNA, with a significantly higher positivity rate in intensive care unit settings (intensive care unit, 27 of 107 [25.2%] vs non-intensive care unit, 39 of 364 [10.7%]; P < .001). There was no difference according to the distance from patients (≤1 m, 3 of 118 [2.5%] vs >1-5 m, 13 of 236 [5.5%]; P = .22). The positivity rate was 5 of 21 air samples (23.8%) in toilets, 20 of 242 (8.3%) in clinical areas, 15 of 122 (12.3%) in staff areas, and 14 of 42 (33.3%) in public areas. A total of 81 viral cultures were performed across 5 studies, and 7 (8.6%) from 2 studies were positive, all from close patient environments. The median (interquartile range) SARS-CoV-2 RNA concentrations varied from 1.0 × 103 copies/m3 (0.4 × 103 to 3.1 × 103 copies/m3) in clinical areas to 9.7 × 103 copies/m3 (5.1 × 103 to 14.3 × 103 copies/m3) in the air of toilets or bathrooms. Protective equipment removal and patient rooms had high concentrations per titer of SARS-CoV-2 (varying from 0.9 × 103 to 40 × 103 copies/m3 and 3.8 × 103 to 7.2 × 103 TCID50/m3), with aerosol size distributions that showed peaks in the region of particle size less than 1 μm; staff offices had peaks in the region of particle size greater than 4 μm.
Conclusions and relevance: In this systematic review, the air close to and distant from patients with coronavirus disease 2019 was frequently contaminated with SARS-CoV-2 RNA; however, few of these samples contained viable viruses. High viral loads found in toilets and bathrooms, staff areas, and public hallways suggest that these areas should be carefully considered.
Conflict of interest statement
Figures
References
-
- World Health Organisation Transmission of SARS-CoV-2: implications for infection prevention precautions. Published online July 9, 2020. Accessed November 23, 2020. https://www.who.int/news-room/commentaries/detail/transmission-of-sars-c...
-
- Birgand G, Mutters NT, Otter JA, et al. Analysis of national and international guidelines on respiratory protection equipment for COVID-19 in healthcare settings. medRxiv. Preprint published online April 29, 2020. doi: 10.1101/2020.04.23.20077230 - DOI
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
