

Blood Pressure and Brain Lesions in Patients With Atrial Fibrillation
- PMID: 33356398
- PMCID: PMC7803457
- DOI: 10.1161/HYPERTENSIONAHA.120.16025
Blood Pressure and Brain Lesions in Patients With Atrial Fibrillation
Abstract
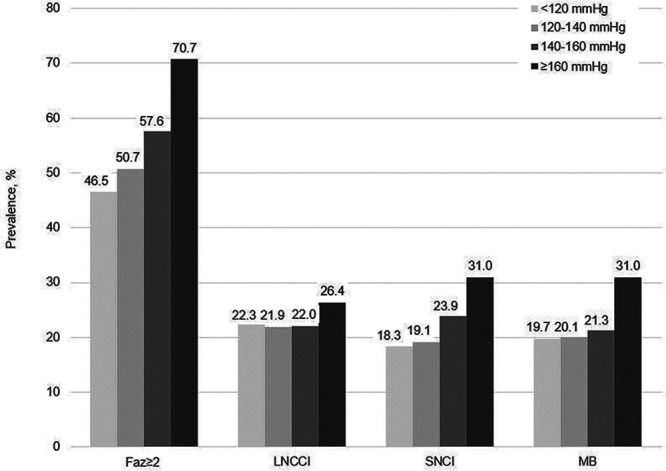
The association of blood pressure (BP) and hypertension with the presence of different types of brain lesions in patients with atrial fibrillation is unclear. BP values were obtained in a multicenter cohort of patients with atrial fibrillation. Systolic and diastolic BP was categorized in predefined groups. All patients underwent brain magnetic resonance imaging and neurocognitive testing. Brain lesions were classified as large noncortical or cortical infarcts, small noncortical infarcts, microbleeds, or white matter lesions. White matter lesions were graded according to the Fazekas scale. Overall, 1738 patients with atrial fibrillation were enrolled in this cross-sectional analysis (mean age, 73 years, 73% males). Mean BP was 135/79 mm Hg, and 67% of participants were taking BP-lowering treatment. White matter lesions Fazekas ≥2 were found in 54%, large noncortical or cortical infarcts in 22%, small noncortical infarcts in 21%, and microbleeds in 22% of patients, respectively. Compared with patients with systolic BP <120 mm Hg, the adjusted odds ratios (95% CI) for Fazekas≥2 was 1.25 (0.94-1.66), 1.41 (1.03-1.93), and 2.54 (1.65-3.95) among patients with systolic BP of 120 to 140, 140 to 160, and ≥160 mm Hg (P for linear trend<0.001). Per 5 mm Hg increase in systolic and diastolic BP, the adjusted β-coefficient (95% CI) for log-transformed white matter lesions was 0.04 (0.02-0.05), P<0.001 and 0.04 (0.01-0.06), P=0.004. Systolic BP was associated with small noncortical infarcts (odds ratios [95% CI] per 5 mm Hg 1.05 [1.01-1.08], P=0.006), microbleeds were associated with hypertension, but large noncortical or cortical infarcts were not associated with BP or hypertension. After multivariable adjustment, BP and hypertension were not associated with neurocognitive function. Among patients with atrial fibrillation, BP is strongly associated with the presence and extent of white matter lesions, but there is no association with large noncortical or cortical infarcts. Registration: URL: https://www.clinicaltrials.gov; Unique identifier: NCT02105844.
Keywords: atrial fibrillation; blood pressure; brain; magnetic resonance imaging; white matter.
Figures


References
-
- Conen D, Ridker PM, Buring JE, Glynn RJ. Risk of cardiovascular events among women with high normal blood pressure or blood pressure progression: prospective cohort study. BMJ. 2007;335:432 doi: 10.1136/bmj.39269.672188.AE - PMC - PubMed
-
- Lewington S, Clarke R, Qizilbash N, Peto R, Collins R; Prospective Studies Collaboration. Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet. 2002;360:1903–1913. doi: 10.1016/s0140-6736(02)11911-8 - PubMed
-
- Rapsomaniki E, Timmis A, George J, Pujades-Rodriguez M, Shah AD, Denaxas S, White IR, Caulfield MJ, Deanfield JE, Smeeth L, et al. Blood pressure and incidence of twelve cardiovascular diseases: lifetime risks, healthy life-years lost, and age-specific associations in 1·25 million people. Lancet. 2014;383:1899–1911. doi: 10.1016/S0140-6736(14)60685-1 - PMC - PubMed
-
- Kearney PM, Whelton M, Reynolds K, Muntner P, Whelton PK, He J. Global burden of hypertension: analysis of worldwide data. Lancet. 2005;365:217–223. doi: 10.1016/S0140-6736(05)17741-1 - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
