

Long-Term Outcomes Among a Nationwide Cohort of Patients Using an Implantable Cardioverter-Defibrillator: UMBRELLA Study Final Results
- PMID: 33356406
- PMCID: PMC7955463
- DOI: 10.1161/JAHA.120.018108
Long-Term Outcomes Among a Nationwide Cohort of Patients Using an Implantable Cardioverter-Defibrillator: UMBRELLA Study Final Results
Abstract
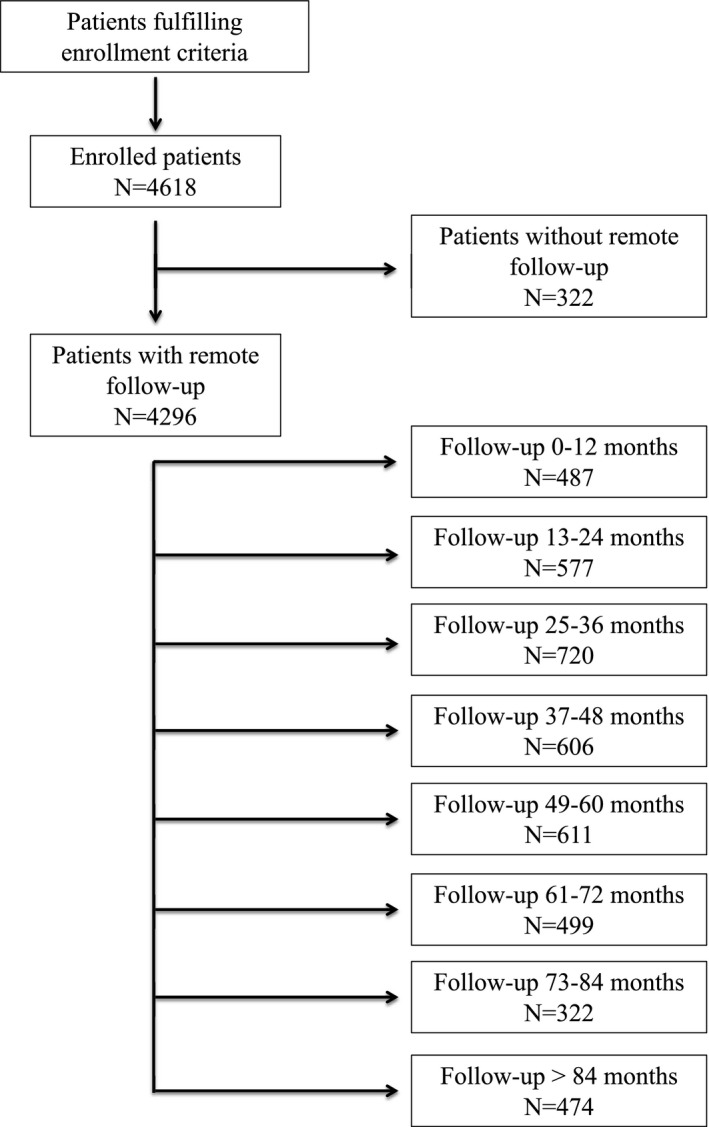
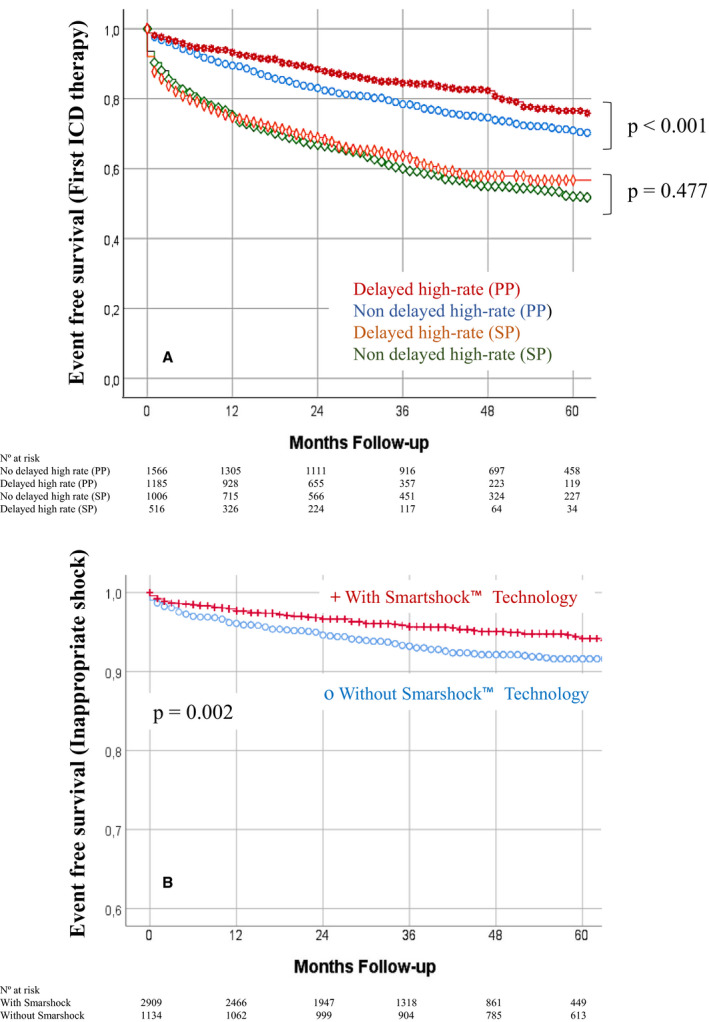
Background Large-scale studies describing modern populations using an implantable cardioverter-defibrillator (ICD) are lacking. We aimed to analyze the incidence of arrhythmia, device interventions, and mortality in a broad spectrum of real-world ICD patients with different heart disorders. Methods and Results The UMBRELLA study is a prospective, multicenter, nationwide study of contemporary patients using an ICD followed up by remote monitoring, with a blinded review of arrhythmic episodes. From November 2005 to November 2017, 4296 patients were followed up. After 46.6±27.3 months, 16 067 episodes of sustained ventricular arrhythmia occurred in 1344 patients (31.3%). Appropriate ICD therapy occurred in 27.3% of study population. Patients with ischemic cardiomyopathy (hazard ratio [HR], 1.51; 95% CI, 1.29-1.78), dilated cardiomyopathy (HR, 1.28; 95% CI, 1.07-1.53), and valvular heart disease (HR, 1.94; 95% CI, 1.43-2.62) exhibited a higher risk of appropriate ICD therapies, whereas patients with hypertrophic cardiomyopathy (HR, 0.72; 95% CI, 0.54-0.96) and Brugada syndrome (HR, 0.25; 95% CI, 0.14-0.45) showed a lower risk. All-cause death was 13.4% at follow-up. Ischemic cardiomyopathy (HR, 3.09; 95% CI, 2.58-5.90), dilated cardiomyopathy (HR, 3.33; 95% CI, 2.18-5.10), and valvular heart disease (HR, 3.97; 95% CI, 2.25-6.99) had the worst prognoses. Delayed high-rate detection was enabled in 39.7% of patients, and single-zone programming occurred in 52.6% of primary prevention patients. Both parameters correlated with lower risk of first appropriate ICD therapy, with no excess risk of mortality. The rate of inappropriate shocks at follow-up was low (6%) and did not differ among type of ICD but was lower in SmartShock-capable devices. Conclusions Irrespective of the cause, contemporary ICD patients with heart failure-related disorders had a similar risk of ICD life-saving interventions and death. Current ICD programming recommendations still need to be implemented. Registration URL: https://www.clinicaltrials.gov; Unique identifier: NTC01561144.
Trial registration: ClinicalTrials.gov NCT01561144.
Keywords: all‐cause death; appropriate implantable cardioverter‐defibrillator therapy; implantable cardioverter‐defibrillator; inappropriate shock; sustained ventricular arrhythmia.
Conflict of interest statement
Dr Briongos‐Figuero reports personal fees and nonfinancial support from Medtronic Iberica and personal fees from Boston Scientific. Dr García‐Alberola reports grants from Medtronic. Dr Rubio reports personal fees from Medtronic, St. Jude, and Boston Scientific. Dr Segura reports personal fees from Medtronic and grants from Boston Scientific. Dr Peinado reports personal fees from Medtronic and grants from Medtronic, Boston Scientific, and Abbot. Dr Martínez‐Ferrer reports personal fees and nonfinancial support from Medtronic. Drs Martín and Cerdá are employees of Medtronic.
Figures

References
-
- Priori SG, Blomstrom‐Lundqvist C, Mazzanti A, Blom N, Borggrefe M, Camm J, Elliott PM, Fitzsimons D, Hatala R, Hindricks G, et al. 2015 ESC guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: the Task Force for the Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death of the Europe. Eur Heart J. 2015;36:2793–2867. - PubMed
-
- O’Mahony C, Jichi F, Pavlou M, Monserrat L, Anastasakis A, Rapezzi C, Biagini E, Gimeno JR, Limongelli G, McKenna WJ, et al. A novel clinical risk prediction model for sudden cardiac death in hypertrophic cardiomyopathy (HCM risk‐SCD). Eur Heart J. 2014;35:2010–2020. - PubMed
-
- Orgeron GM, James CA, Te RA, Tichnell C, Murray B, Bhonsale A, Kamel IR, Zimmerman SL, Judge DP, Crosson J, et al. Implantable cardioverter‐defibrillator therapy in arrhythmogenic right ventricular dysplasia/cardiomyopathy: predictors of appropriate therapy, outcomes, and complications. J Am Heart Assoc. 2017;6:e006242. DOI: 10.1161/JAHA.117.006242. - DOI - PMC - PubMed
-
- Schwartz PJ, Spazzolini C, Priori SG, Crotti L, Vicentini A, Landolina M, Gasparini M, Wilde AAM, Knops RE, Denjoy I, et al. Who are the long‐QT syndrome patients who receive an implantable cardioverter‐defibrillator and what happens to them? Data from the European Long‐QT Syndrome Implantable Cardioverter‐Defibrillator (LQTS ICD) Registry. Circulation. 2010;122:1272–1282. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
