

Primary adrenal insufficiency due to adrenal tuberculosis: a case report
- PMID: 33356711
- PMCID: PMC7768570
- DOI: 10.1177/0300060520980590
Primary adrenal insufficiency due to adrenal tuberculosis: a case report
Abstract
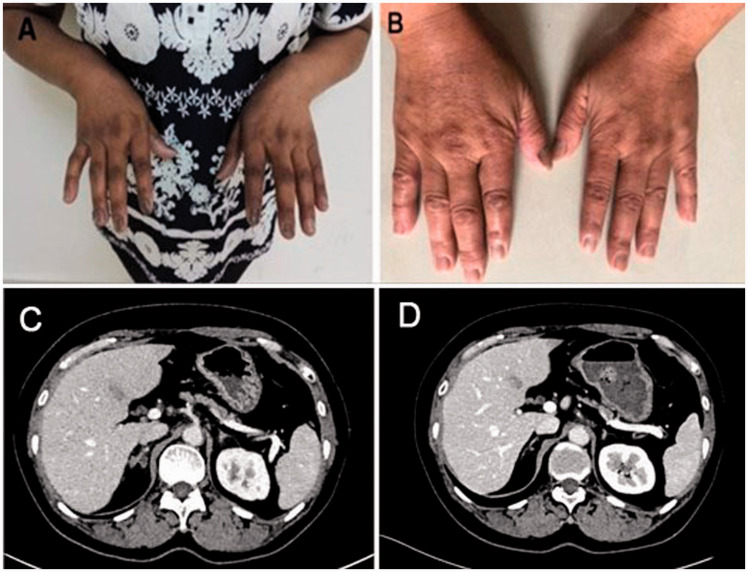
We report a case of primary adrenal insufficiency (PAI) due to adrenal tuberculosis with no findings of active tuberculosis in the lung of a 51-year-old female patient. The patient was admitted with a 10-year history of skin hyperpigmentation and was diagnosed with PAI. The primary cause was adrenal tuberculosis. An adrenocorticotropic hormone stimulation test, T-Spot test and adrenal computed tomography scan were used to confirm the diagnosis. The patient's status improved, and the hyperpigmentation subsided after 15 months of treatment with anti-tuberculosis drugs and cortisol replacement therapy.
Keywords: Primary adrenal insufficiency; adrenal tuberculosis; autoimmune adrenal disease; cortisol replacement therapy; extra-pulmonary tuberculosis; hyperpigmentation.
Conflict of interest statement
Figures
Similar articles
-
Autoimmune Primary Adrenal Insufficiency in Children.J Clin Res Pediatr Endocrinol. 2022 Aug 25;14(3):308-312. doi: 10.4274/jcrpe.galenos.2022.2021-11-9. Epub 2022 May 31. J Clin Res Pediatr Endocrinol. 2022. PMID: 35633647 Free PMC article.
-
New-Onset Primary Adrenal Insufficiency and Autoimmune Hypothyroidism in a Pediatric Patient Presenting with MIS-C.Horm Res Paediatr. 2022;95(4):397-401. doi: 10.1159/000525227. Epub 2022 May 24. Horm Res Paediatr. 2022. PMID: 35609533 Free PMC article.
-
Adrenal insufficiency following nivolumab therapy in patients with recurrent or metastatic head and neck cancer.Auris Nasus Larynx. 2020 Apr;47(2):309-313. doi: 10.1016/j.anl.2019.05.009. Epub 2019 Jun 22. Auris Nasus Larynx. 2020. PMID: 31235078
-
Adrenal crisis provoked by dental infection: case report and review of the literature.Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010 Sep;110(3):325-9. doi: 10.1016/j.tripleo.2010.04.025. Epub 2010 Jul 31. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010. PMID: 20674414 Review.
-
Primary adrenal insufficiency in children: Diagnosis and management.Best Pract Res Clin Endocrinol Metab. 2018 Aug;32(4):397-424. doi: 10.1016/j.beem.2018.05.010. Epub 2018 Jun 6. Best Pract Res Clin Endocrinol Metab. 2018. PMID: 30086866 Review.
Cited by
-
Primary adrenal tuberculosis infection in patients with Behcet's disease presenting as isolated adrenal metastasis by 18F-FDG PET/CT: a rare case report and literature review.Gland Surg. 2021 Dec;10(12):3431-3442. doi: 10.21037/gs-21-511. Gland Surg. 2021. PMID: 35070903 Free PMC article.
-
Adrenal Abscesses: A Systematic Review of the Literature.J Clin Med. 2023 Jul 11;12(14):4601. doi: 10.3390/jcm12144601. J Clin Med. 2023. PMID: 37510716 Free PMC article. Review.
-
Complete recovery after glucocorticoid replacement therapy in a case of primary adrenal insufficiency caused by adrenal tuberculosis infection.Endocrinol Diabetes Metab Case Rep. 2023 Dec 13;2023(4):23-0112. doi: 10.1530/EDM-23-0112. Print 2023 Oct 1. Endocrinol Diabetes Metab Case Rep. 2023. PMID: 38088358 Free PMC article.
-
An autopsy case of unexpected death due to Addison's disease caused by adrenal tuberculosis.Eur J Med Res. 2021 Dec 4;26(1):137. doi: 10.1186/s40001-021-00611-w. Eur J Med Res. 2021. PMID: 34863306 Free PMC article.
References
-
- Puar TH, Stikkelbroeck NM, Smans LC, et al. . Adrenal Crisis: Still a Deadly Event in the 21st Century. Am J Med 2016; 129: 339.e1-9. - PubMed
-
- Higuchi K, Sekiya Y, Igari H, et al. Comparison of specificities between two interferon-gamma release assays in Japan. Int J Tuberc Lung Dis 2012; 16: 1190–1192. - PubMed
-
- Takasaki J, Manabe T, Morino E, et al. Sensitivity and specificity of QuantiFERON-TB Gold Plus compared with QuantiFERON-TB Gold In-Tube and T-SPOT.TB on active tuberculosis in Japan. J Infect Chemother 2018; 24: 188–192. - PubMed
-
- Yang C, Zhang S, Yao L, et al. Evaluation of risk factors for false-negative results with an antigen-specific peripheral blood-based quantitative T cell assay (T-SPOT(®). TB) in the diagnosis of active tuberculosis: A large-scale retrospective study in China. J Int Med Res 2018; 46: 1815–1825. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
