

Comparison of Critical Care Occupancy and Outcomes of Critically Ill Patients during the 2020 COVID-19 Winter Surge and 2009 H1N1 Influenza Pandemic in Australia
- PMID: 33356988
- PMCID: PMC8513663
- DOI: 10.1513/AnnalsATS.202010-1311OC
Comparison of Critical Care Occupancy and Outcomes of Critically Ill Patients during the 2020 COVID-19 Winter Surge and 2009 H1N1 Influenza Pandemic in Australia
Abstract
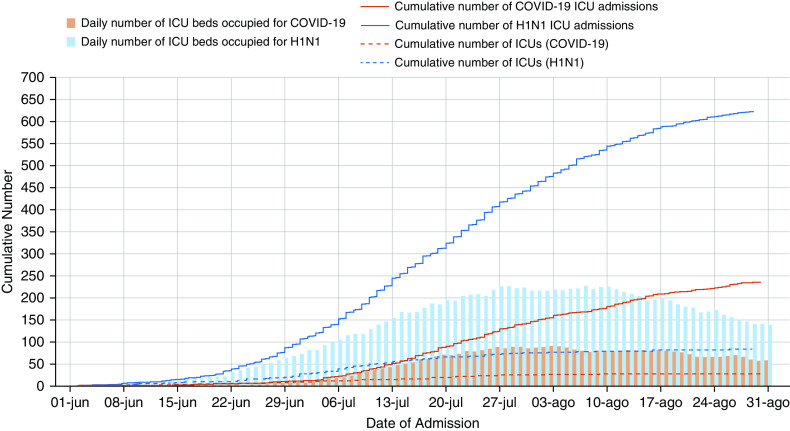
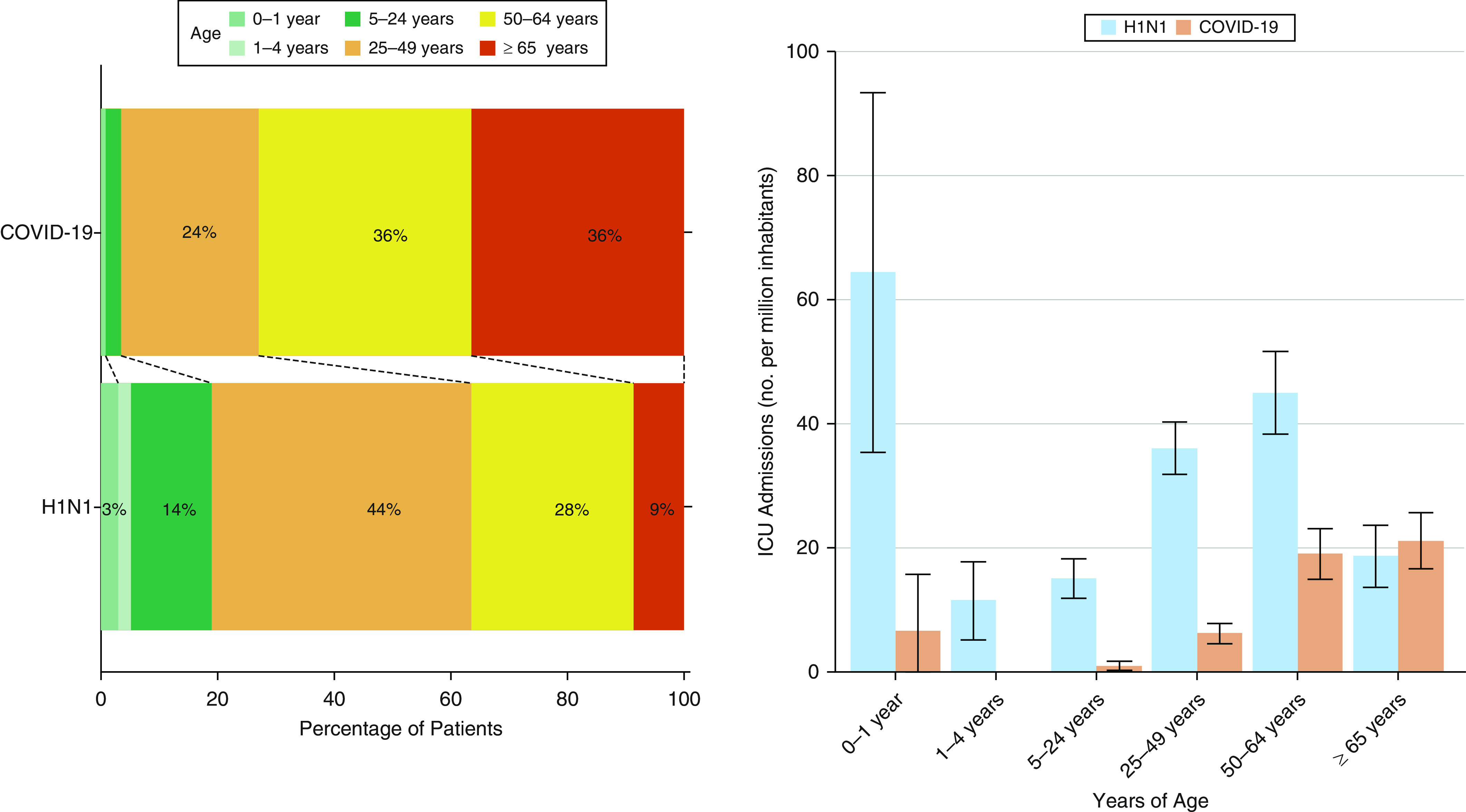
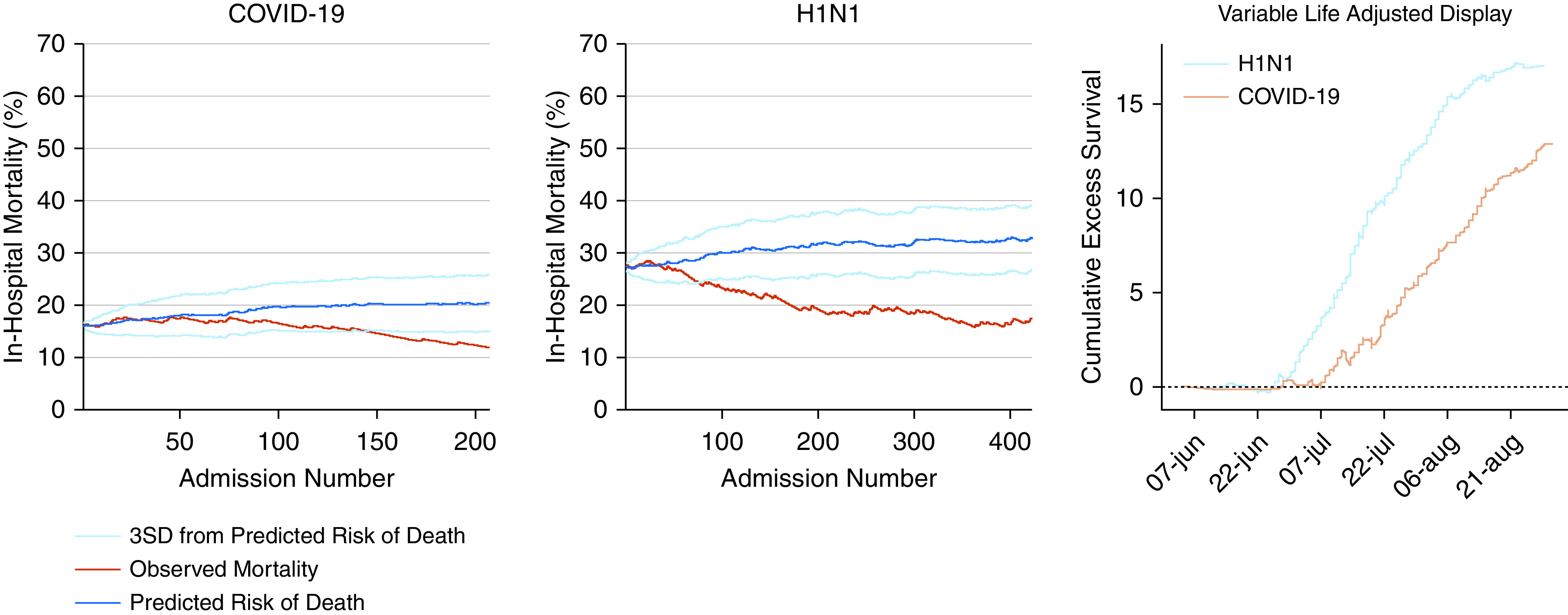
Rationale: Both 2009 pandemic influenza A (H1N1) and severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) are transmitted by respiratory secretions and in severe cases result in a viral pneumonitis, requiring intensive care unit (ICU) admission. However, no studies have compared the clinical characteristics and outcomes of such patients. Objectives: To report and compare the demographic characteristics, treatments, use of critical care resources, and outcomes of patients admitted to an Australian ICU with H1N1 influenza during the winter of 2009, and SARS-CoV-2 during the winter of 2020. Methods: This was a multicenter project, using national data from previous and ongoing epidemiological studies concerning severe acute respiratory infections in Australia. All ICUs admitting patients with H1N1 or coronavirus disease (COVID-19) were included and contributed data. We compared clinical characteristics and outcomes of patients with H1N1 admitted to ICU in the winter of 2009 versus patients with COVID-19 admitted to ICU in the winter of 2020. The primary outcome was in-hospital mortality. Potential years of life lost (PYLL) were calculated according to sex-adjusted life expectancy in Australia. Results: Across the two epochs, 861 patients were admitted to ICUs; 236 (27.4%) with COVID-19 and 625 (72.6%) with H1N1 influenza. The number of ICU admissions and bed-days occupied were higher with 2009 H1N1 influenza. Patients with COVID-19 were older, more often male and overweight, and had lower Acute Physiology and Chronic Health Evaluation II scores at ICU admission. The highest age-specific incidence of ICU admission was among infants (0-1 yr of age) for H1N1, and among the elderly (≥65 yr) for COVID-19. Unadjusted in-hospital mortality was similar (11.5% in COVID-19 vs. 16.1% in H1N1; odds ratio, 0.68 [95% confidence interval (95% CI), 0.42-1.06]; P = 0.10). The PYLL was greater with H1N1 influenza than with COVID-19 at 154.1 (95% CI, 148.7-159.4) versus 13.6 (95% CI, 12.2-15.1) PYLL per million inhabitants. Conclusions: In comparison with 2009 H1N1 influenza, COVID-19 admissions overwinter in Australia resulted in fewer ICU admissions, and lower bed-day occupancy. Crude in-hospital mortality was similar, but because of demographic differences in affected patients, deaths due to 2009 H1N1 influenza led to an 11-fold increase in the number of PYLL in critically ill patients.
Keywords: Australia; COVID-19; H1N1; outcomes; pandemic.
Figures
Comment in
-
COVID-19 Is Not Comparable to H1N1 Influenza.Ann Am Thorac Soc. 2022 Mar;19(3):509-510. doi: 10.1513/AnnalsATS.202110-1097LE. Ann Am Thorac Soc. 2022. PMID: 34818143 Free PMC article. No abstract available.
References
-
- Centers for Disease Control and Prevention H1N1 flu: international situation update Atlanta, GA: Centers for Disease Control and Prevention; 2009[accessed 2009 Oct 19]. Available from: http://www.cdc.gov/h1n1flu/ updates/international/
-
- Webb SA, Pettilä V, Seppelt I, Bellomo R, Bailey M, Cooper DJ, et al. ANZIC Influenza Investigators. Critical care services and 2009 H1N1 influenza in Australia and New Zealand. N Engl J Med. 2009;361:1925–1934. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
