

Multi-organ point-of-care ultrasound for COVID-19 (PoCUS4COVID): international expert consensus
- PMID: 33357240
- PMCID: PMC7759024
- DOI: 10.1186/s13054-020-03369-5
Multi-organ point-of-care ultrasound for COVID-19 (PoCUS4COVID): international expert consensus
Abstract
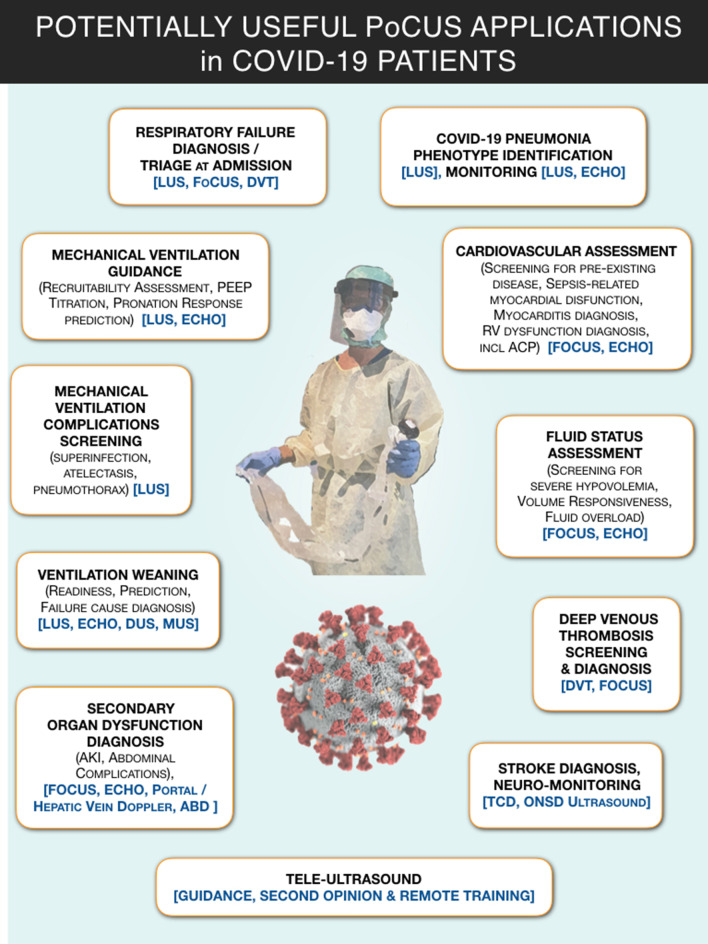
COVID-19 has caused great devastation in the past year. Multi-organ point-of-care ultrasound (PoCUS) including lung ultrasound (LUS) and focused cardiac ultrasound (FoCUS) as a clinical adjunct has played a significant role in triaging, diagnosis and medical management of COVID-19 patients. The expert panel from 27 countries and 6 continents with considerable experience of direct application of PoCUS on COVID-19 patients presents evidence-based consensus using GRADE methodology for the quality of evidence and an expedited, modified-Delphi process for the strength of expert consensus. The use of ultrasound is suggested in many clinical situations related to respiratory, cardiovascular and thromboembolic aspects of COVID-19, comparing well with other imaging modalities. The limitations due to insufficient data are highlighted as opportunities for future research.
Keywords: COVID-19; Echocardiography; Focused cardiac ultrasound (FoCUS); Lung ultrasound (LUS); Point-of-care ultrasound (PoCUS); SARS-CoV-2.
Conflict of interest statement
Except for the following authors, none have declared any disclosures with respect to the present work: A Hussain: Currently serving President of WINFOCUS—G Tavazzi: Received fees for lectures from GE Healthcare unrelated to this work—R Hoppmann: EchoNous Advisory Board—F Mojoli: Received fees for lectures from Hamilton Medical, GE Healthcare, Seda Spa and institutional relationship between University of Pavia and Hamilton Medical—G Via: eMedical Academy co-founder—B Nelson: Echonous and DiA Advisory Board.
Figures
References
-
- Coronavirus disease 2019 (COVID-19) Situation Report – 92 [https://www.who.int/docs/default-source/coronaviruse/situation-reports/2...]
-
- Wu Z, McGoogan JM. Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72314 Cases From the Chinese Center for Disease Control and Prevention. JAMA 2020. - PubMed
-
- Clinical management of severe acute respiratory infection when COVID-19 is suspected - Interim guidance. https://www.who.int/publications-detail/clinical-management-of-severe-ac...
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
