

The Effects of a Multifaceted Intervention to Improve Care Transitions Within an Accountable Care Organization: Results of a Stepped-Wedge Cluster-Randomized Trial
- PMID: 33357325
- PMCID: PMC7768916
- DOI: 10.12788/jhm.3513
The Effects of a Multifaceted Intervention to Improve Care Transitions Within an Accountable Care Organization: Results of a Stepped-Wedge Cluster-Randomized Trial
Abstract
Background: Transitions from hospital to the ambulatory setting are high risk for patients in terms of adverse events, poor clinical outcomes, and readmission.
Objectives: To develop, implement, and refine a multifaceted care transitions intervention and evaluate its effects on postdischarge adverse events.
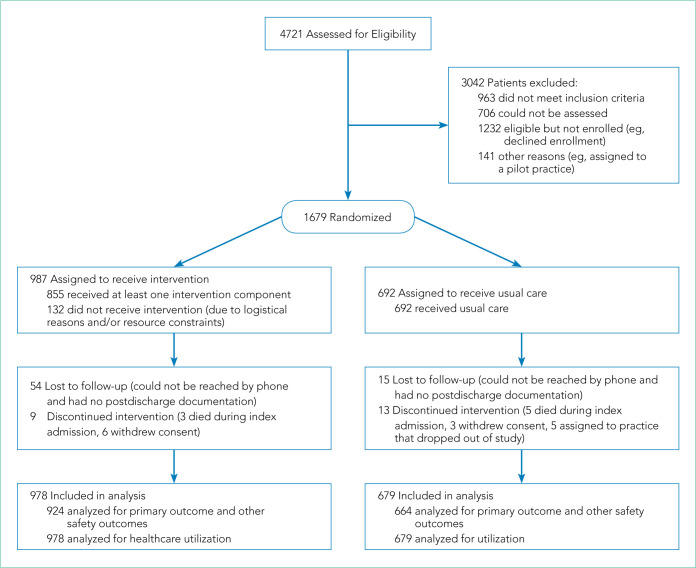
Design, setting, and participants: Two-arm, single-blind (blinded outcomes assessor), stepped-wedge, cluster-randomized clinical trial. Participants were 1,679 adult patients who belonged to one of 17 primary care practices and were admitted to a medical or surgical service at either of two participating hospitals within a pioneer accountable care organization (ACO).
Interventions: Multicomponent intervention in the 30 days following hospitalization, including inpatient pharmacist-led medication reconciliation, coordination of care between an inpatient "discharge advocate" and a primary care "responsible outpatient clinician," postdischarge phone calls, and postdischarge primary care visit.
Main outcomes and measures: The primary outcome was rate of postdischarge adverse events, as assessed by a 30-day postdischarge phone call and medical record review and adjudicated by two blinded physician reviewers. Secondary outcomes included preventable adverse events, new or worsening symptoms after discharge, and 30-day nonelective hospital readmission.
Results: Among patients included in the study, 692 were assigned to usual care and 987 to the intervention. Patients in the intervention arm had a 45% relative reduction in postdischarge adverse events (18 vs 23 events per 100 patients; adjusted incidence rate ratio, 0.55; 95% CI, 0.35-0.84). Significant reductions were also seen in preventable adverse events and in new or worsening symptoms, but there was no difference in readmission rates.
Conclusion: A multifaceted intervention was associated with a significant reduction in postdischarge adverse events but no difference in 30-day readmission rates.
Keywords: Care transition; Care coordination; Readmission; Discharge planning; Discharge process; Interdisciplinary communication; Medication reconciliation; Medication education.
Figures
Comment in
-
Care Transitions: A Complex Problem That Requires a Complexity Mindset.J Hosp Med. 2021 Jan;16(1):62. doi: 10.12788/jhm.3534. J Hosp Med. 2021. PMID: 33357334 No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
