

Outcomes of paediatric patients with B-cell acute lymphocytic leukaemia with ABL-class fusion in the pre-tyrosine-kinase inhibitor era: a multicentre, retrospective, cohort study
- PMID: 33357483
- PMCID: PMC9709453
- DOI: 10.1016/S2352-3026(20)30353-7
Outcomes of paediatric patients with B-cell acute lymphocytic leukaemia with ABL-class fusion in the pre-tyrosine-kinase inhibitor era: a multicentre, retrospective, cohort study
Erratum in
-
Correction to Lancet Haematol 2021; 8: e55-66.Lancet Haematol. 2021 Nov;8(11):e789. doi: 10.1016/S2352-3026(21)00310-0. Lancet Haematol. 2021. PMID: 34715046 No abstract available.
Abstract
Background: ABL-class fusion genes other than BCR-ABL1 have been identified in approximately 3% of children with newly diagnosed acute lymphocytic leukaemia, and studies suggest that leukaemic cells carrying ABL-class fusions can be targeted successfully by tyrosine-kinase inhibitors. We aimed to establish the baseline characteristics and outcomes of paediatric patients with ABL-class fusion B-cell acute lymphocytic leukaemia in the pre-tyrosine-kinase inhibitor era.
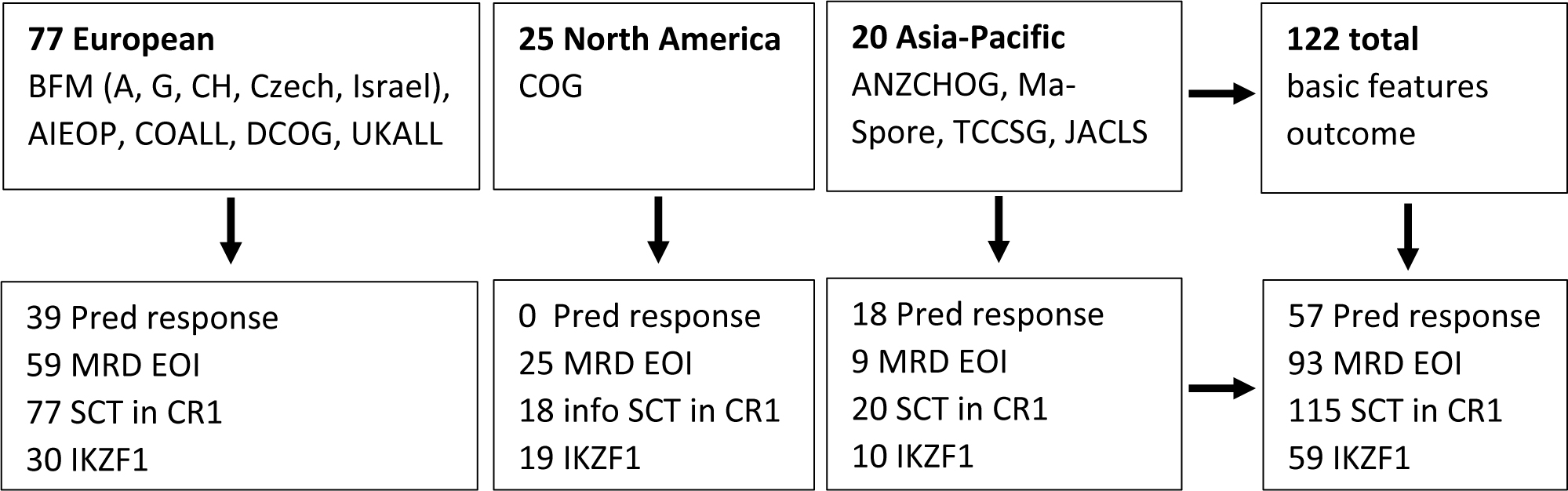
Methods: This multicentre, retrospective, cohort study included paediatric patients (aged 1-18 years) with newly diagnosed ABL-class fusion (ABL1 fusion-positive, ABL2 fusion-positive, CSF1R fusion-positive, and PDGFRB fusion-positive) B-cell acute lymphocytic leukaemia enrolled in clinical trials of multidrug chemotherapy done between Oct 3, 2000, and Aug 28, 2018, in which tyrosine-kinase inhibitors had not been given as a first-line treatment. Patients from 14 European, North American, and Asia-Pacific study groups of the Ponte di Legno group were included. No patients were excluded, and patients were followed up by individual study groups. Through the Ponte di Legno group, we collected data on the baseline characteristics of patients, including IKZF1, PAX5, and CDKN2A/B deletion status, and whether haematopoietic stem cell transplantation (HSCT) had been done, as well as treatment outcomes, including complete remission, no response, relapse, early death, and treatment-related mortality, response to prednisone, and minimal residual disease (MRD) at end of induction therapy. 5-year event-free survival and 5-year overall survival were estimated by use of Kaplan-Meier methods, and the 5-year cumulative incidence of relapse was calculated by use of a competing risk model.
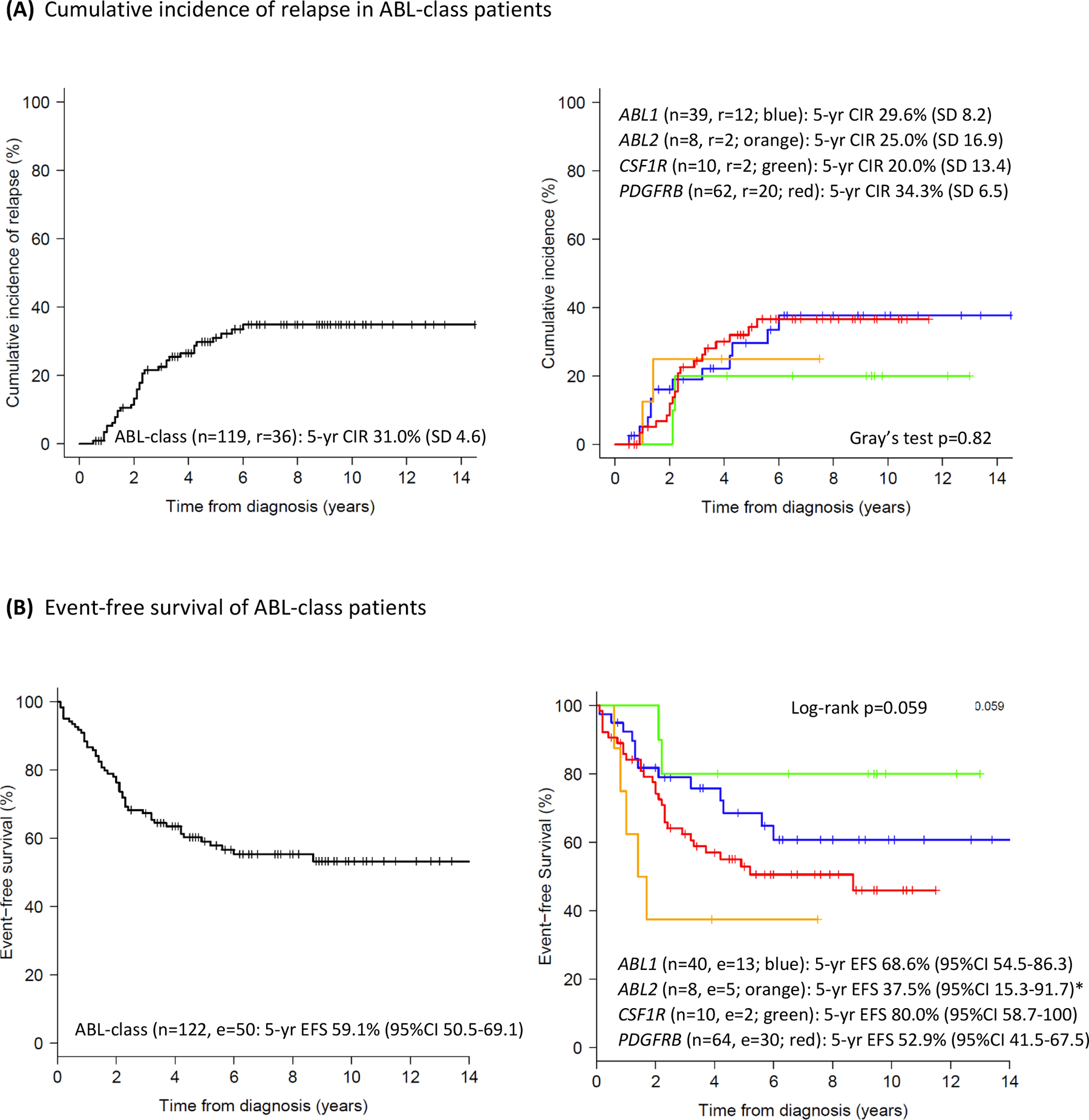
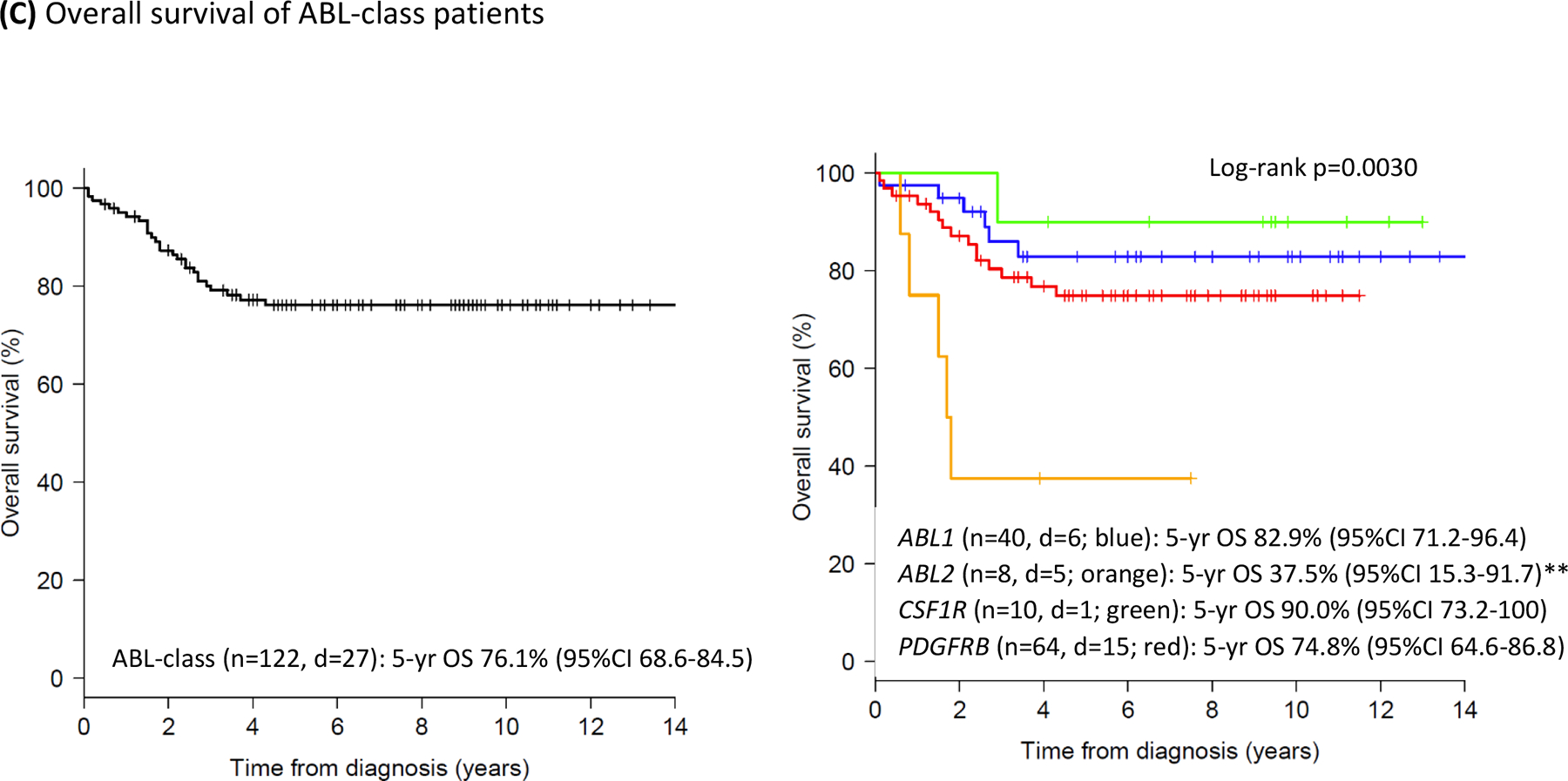
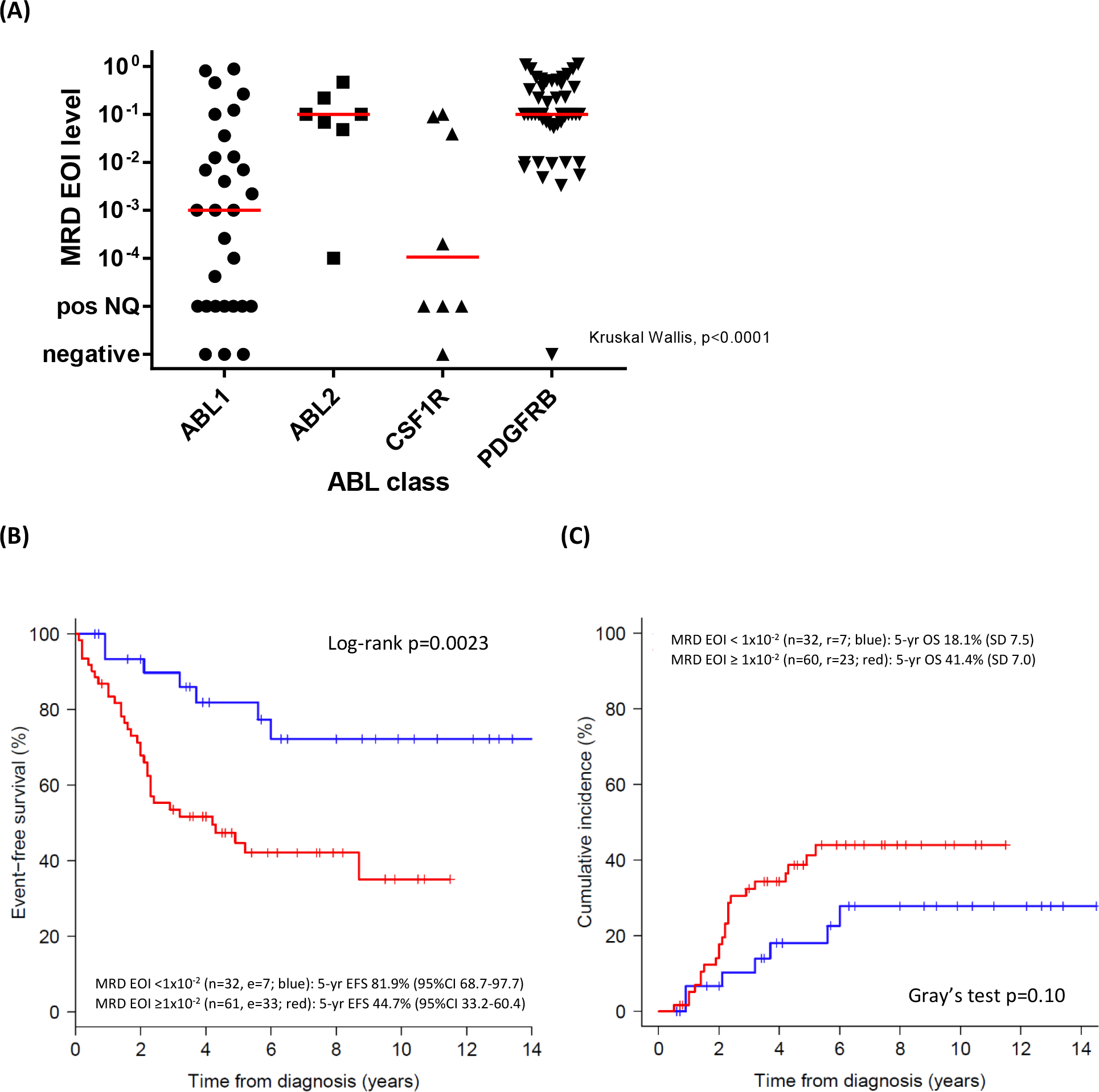
Findings: We identified 122 paediatric patients with newly diagnosed ABL-class fusion B-cell acute lymphocytic leukaemia (77 from European study groups, 25 from North American study groups, and 20 from Asia-Pacific study groups). 64 (52%) of 122 patients were PDGFRB fusion-positive, 40 (33%) were ABL1 fusion-positive, ten (8%) were CSF1R fusion-positive, and eight (7%) were ABL2 fusion-positive. In all 122 patients, 5-year event-free survival was 59·1% (95% CI 50·5-69·1), 5-year overall survival was 76·1% (68·6-84·5), and the 5-year cumulative incidence of relapse was 31·0% (95% CI 22·4-40·1). MRD at the end of induction therapy was high (≥10-2 cells) in 61 (66%) of 93 patients, and most prevalent in patients with ABL2 fusions (six [86%] of 7 patients) and PDGFRB fusion-positive B-cell acute lymphocytic leukaemia (43 [88%] of 49 patients). MRD at the end of induction therapy of 10-2 cells or more was predictive of an unfavourable outcome (hazard ratio of event-free survival in patients with a MRD of ≥10-2vs those with a MRD of <10-2 3·33 [95% CI 1·46-7·56], p=0·0039). Of the 36 (30%) of 119 patients who relapsed, 25 (69%) relapsed within 3 years of diagnosis. The 5-year cumulative incidence of relapse in 41 patients who underwent HSCT (17·8% [95% CI 7·7-31·3]) was lower than in the 43 patients who did not undergo HSCT (45·1% [28·4-60·5], p=0·013), but event-free survival and overall survival did not differ between these two groups.
Interpretation: Children with ABL-class fusion B-cell acute lymphocytic leukaemia have poor outcomes when treated with regimens that do not contain a tyrosine-kinase inhibitor, despite the use of high-risk chemotherapy regimens and frequent HSCT upon first remission. Our findings provide a reference for evaluating the potential benefit of first-line tyrosine-kinase inhibitor treatment in patients with ABL-class fusion B-cell acute lymphocytic leukaemia.
Funding: The Oncode Institute, Pediatric Cancer Foundation Rotterdam, Dutch Cancer Society, Kika Foundation, Deutsche Krebshilfe, Blood Cancer UK, Associazione Italiana per la Ricerca sul Cancro, Cancer Australia, National Cancer Institute, National Institute of Health, and St Baldrick's Foundation.
Copyright © 2021 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interest
MLdB, AVM, HAdGK, JMB, MF, GE, TI, AY, RS, LDP, NK, KGR, AV, AA, MZ, SE, GCazzaniga, AB, MLL and RP declare no competing interests. GCario reports personal fees from Jazz Pharmaceuticals and Novartis outside the submitted work. SPH reports personal fees from Novartis, Amgen, and other from Amgen, outside the submitted work. CGM reports personal fees from Illumina and grants from Loxo Oncology during the conduct of the study, and grants from Abbvie and Pfizer and personal fees from Amgen outside the submitted work. MS reports grants from SHIRE, JazzPharma, Servier, SigmaTau, Amgen, and Novartis during the conduct of the study, and personal fees from SHIRE, Servier, and JazzPharma outside the submitted work.
Figures
Comment in
-
Are we ABL to do better for children with BCR-ABL1-like acute lymphocytic leukaemia?Lancet Haematol. 2021 Jan;8(1):e6-e8. doi: 10.1016/S2352-3026(20)30362-8. Epub 2020 Dec 22. Lancet Haematol. 2021. PMID: 33357484 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
