

A multi-center study on safety and efficacy of immune checkpoint inhibitors in cancer patients with kidney transplant
- PMID: 33359528
- PMCID: PMC8222056
- DOI: 10.1016/j.kint.2020.12.015
A multi-center study on safety and efficacy of immune checkpoint inhibitors in cancer patients with kidney transplant
Abstract
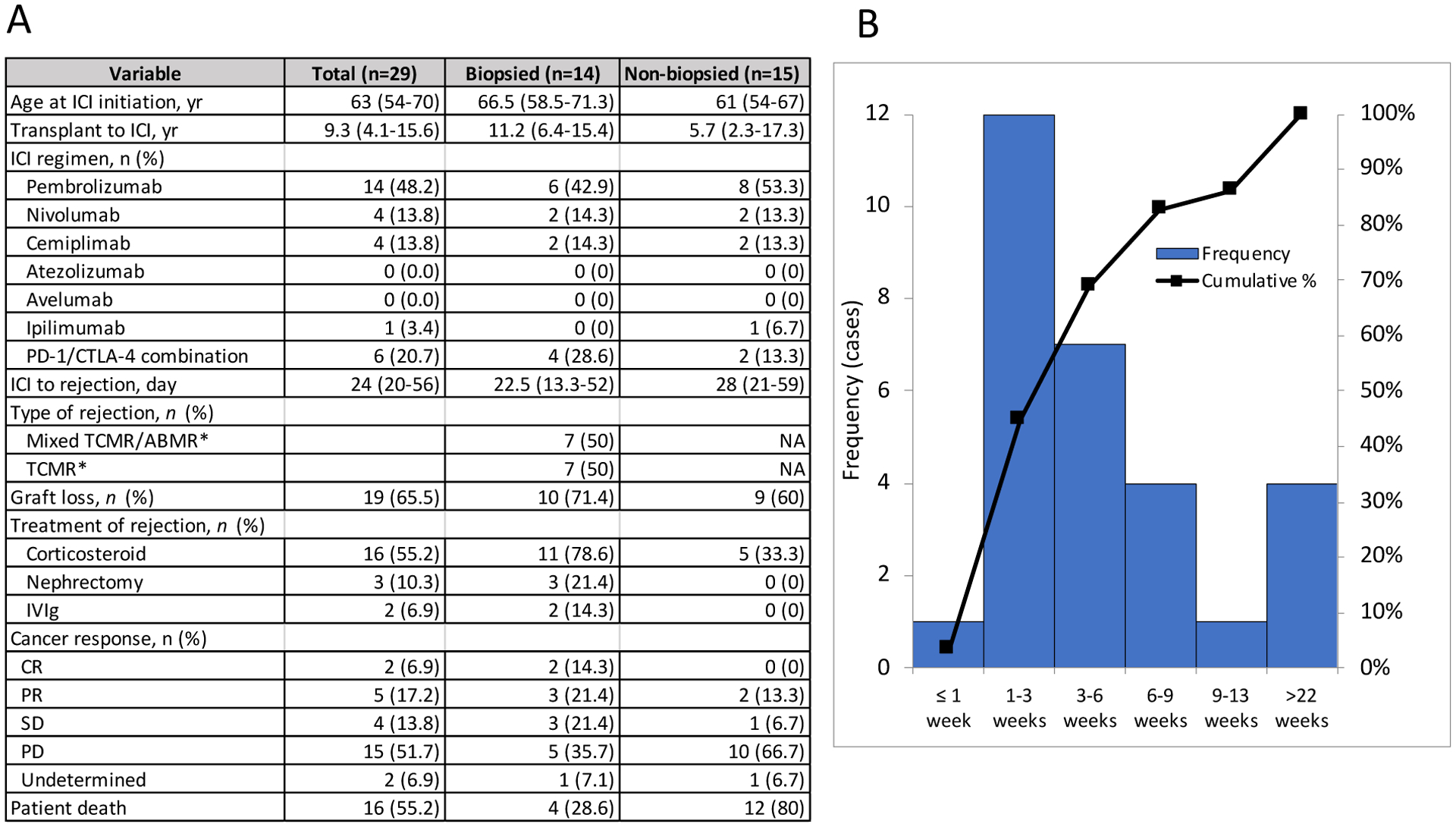
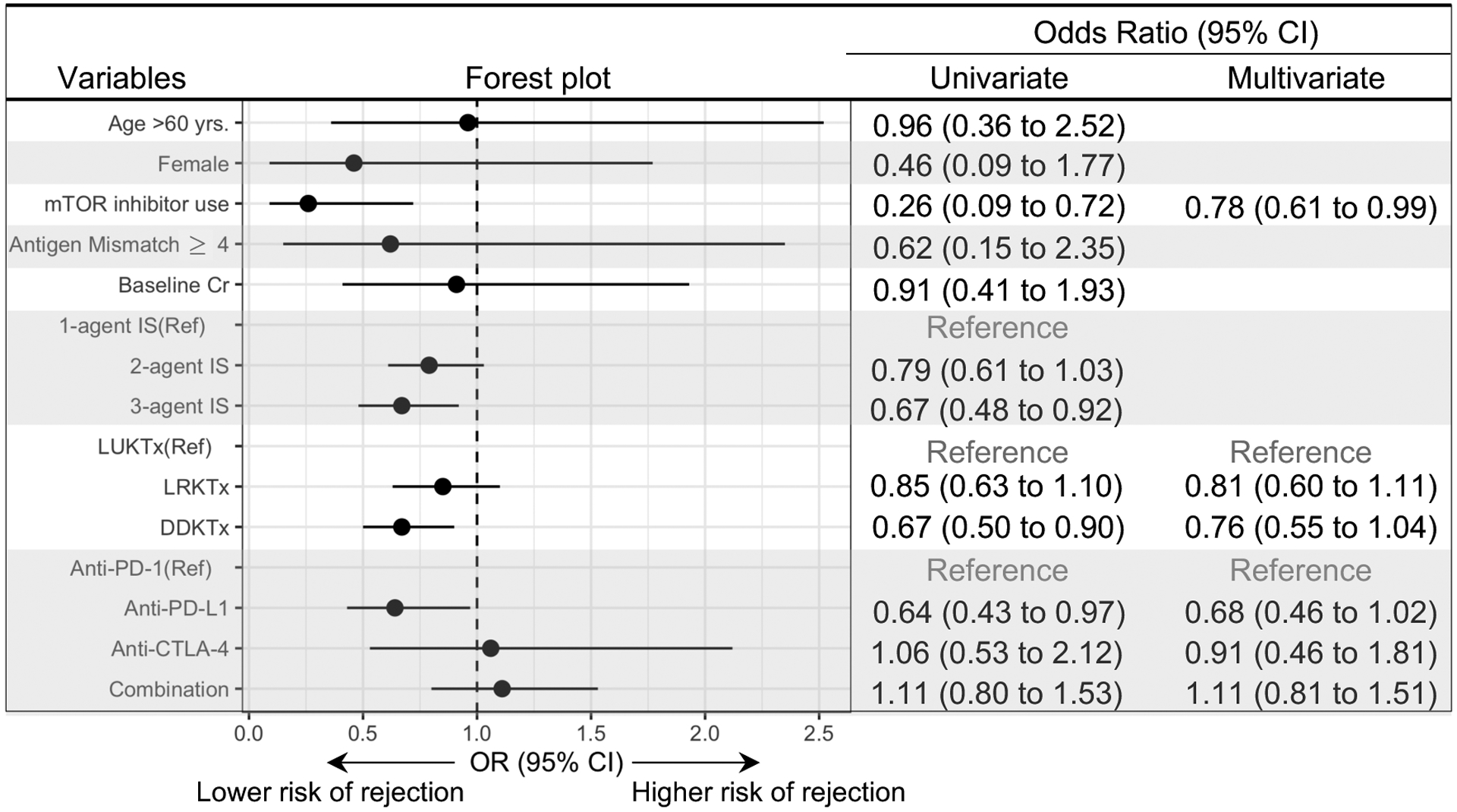
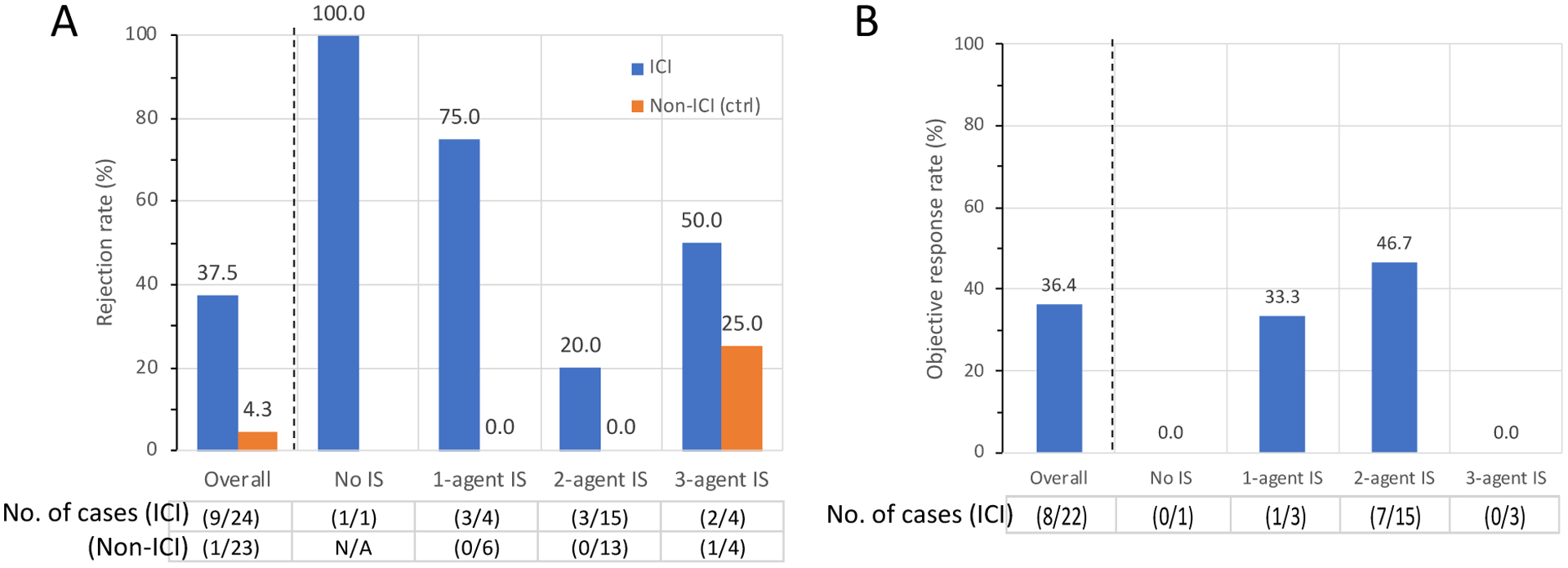
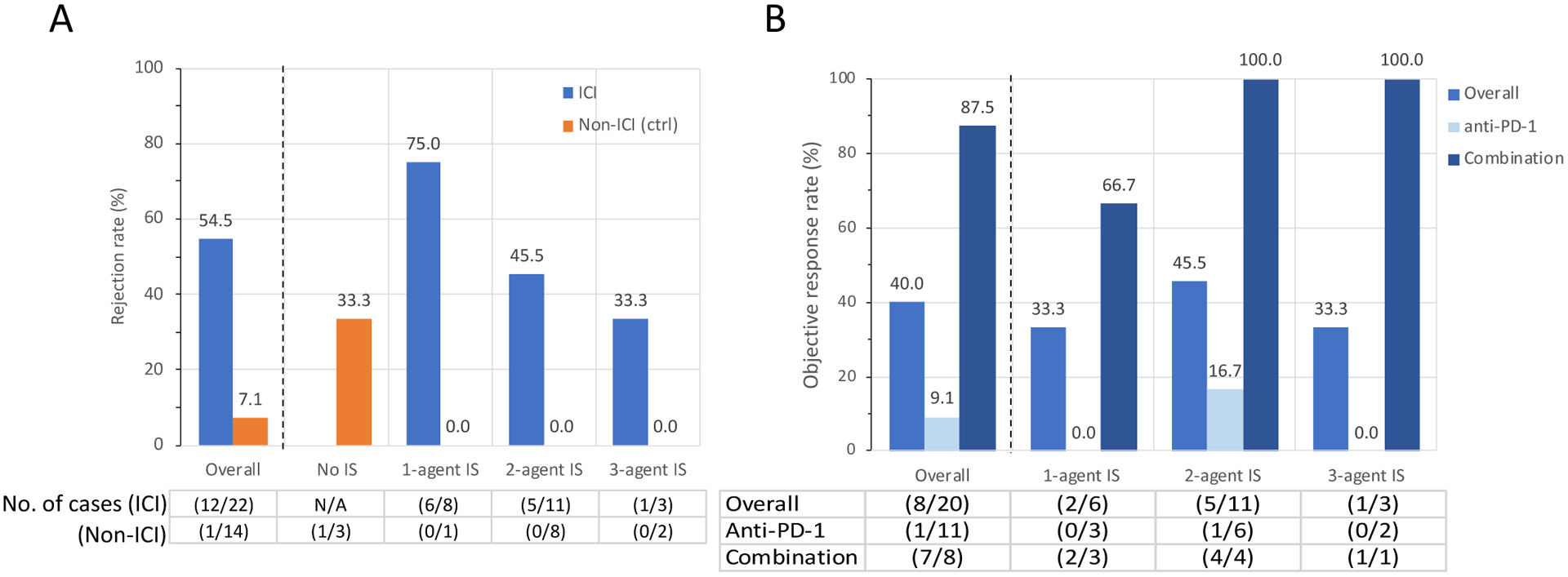
Immune checkpoint inhibitors (ICIs) are widely used for various malignancies. However, their safety and efficacy in patients with a kidney transplant have not been defined. To delineate this, we conducted a multicenter retrospective study of 69 patients with a kidney transplant receiving ICIs between January 2010 and May 2020. For safety, we assessed the incidence, timing, and risk factors of acute graft rejection. For efficacy, objective response rate and overall survival were assessed in cutaneous squamous cell carcinoma and melanoma, the most common cancers in our cohort, and compared with stage-matched 23 patients with squamous cell carcinoma and 14 with melanoma with a kidney transplant not receiving ICIs. Following ICI treatment, 29 out of 69 (42%) patients developed acute rejection, 19 of whom lost their allograft, compared with an acute rejection rate of 5.4% in the non-ICI cohort. Median time from ICI initiation to rejection was 24 days. Factors associated with a lower risk of rejection were mTOR inhibitor use (odds ratio 0.26; 95% confidence interval, 0.09-0.72) and triple-agent immunosuppression (0.67, 0.48-0.92). The objective response ratio was 36.4% and 40% in the squamous cell carcinoma and melanoma subgroups, respectively. In the squamous cell carcinoma subgroup, overall survival was significantly longer in patients treated with ICIs (median overall survival 19.8 months vs. 10.6 months), whereas in the melanoma subgroup, overall survival did not differ between groups. Thus, ICIs were associated with a high risk of rejection in patients with kidney transplants but may lead to improved cancer outcomes. Prospective studies are needed to determine optimal immunosuppression strategies to improve patient outcomes.
Keywords: immune checkpoint inhibitors; kidney transplant; onconephrology; rejection.
Copyright © 2020 International Society of Nephrology. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Sharma P, Allison JP: The future of immune checkpoint therapy. Science 348:56–61, 2015 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
