

Patient-centered contrast thresholds to reduce acute kidney injury in high-risk patients undergoing percutaneous coronary intervention
- PMID: 33359778
- PMCID: PMC7954906
- DOI: 10.1016/j.ahj.2020.12.013
Patient-centered contrast thresholds to reduce acute kidney injury in high-risk patients undergoing percutaneous coronary intervention
Abstract
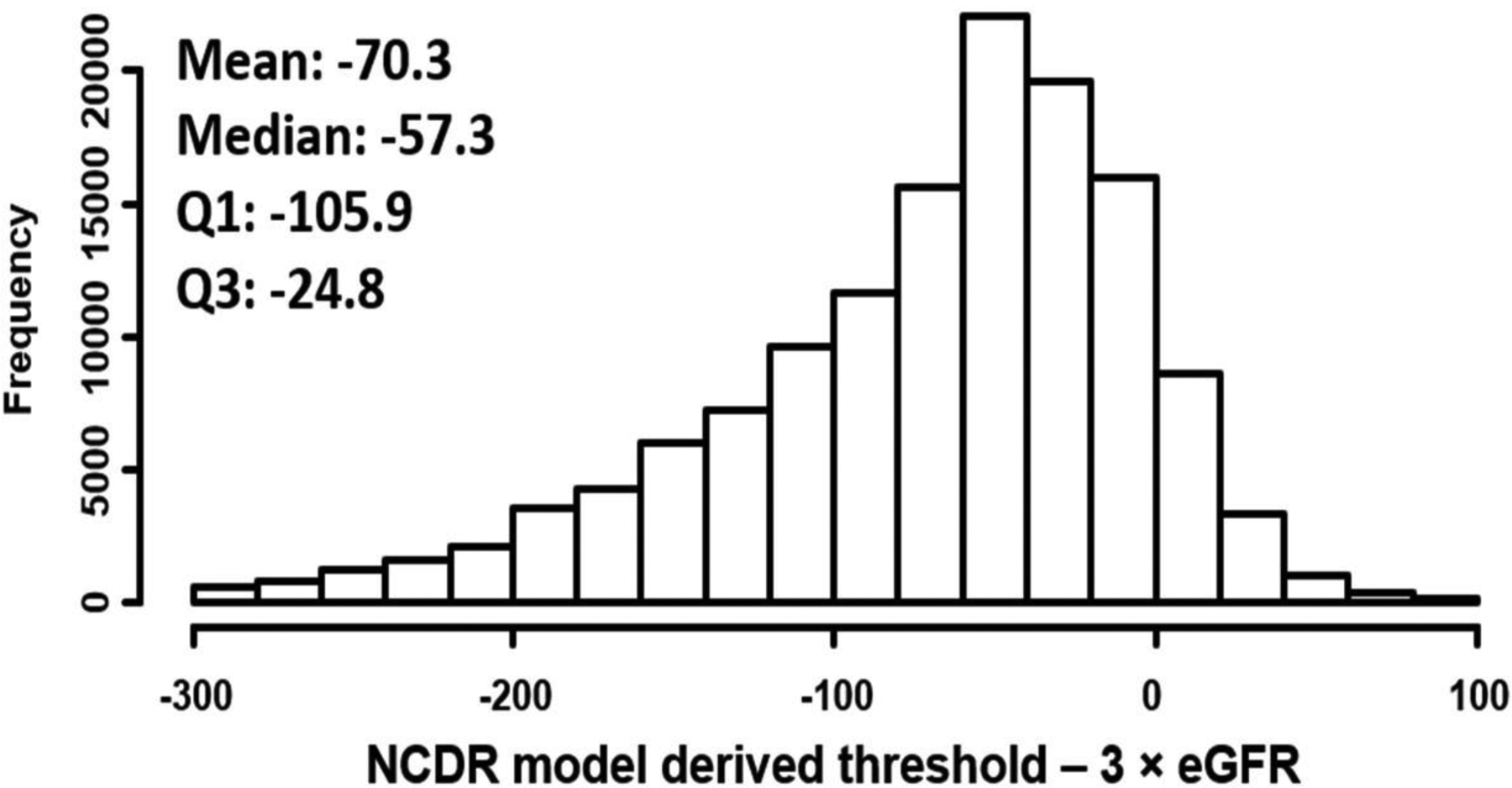
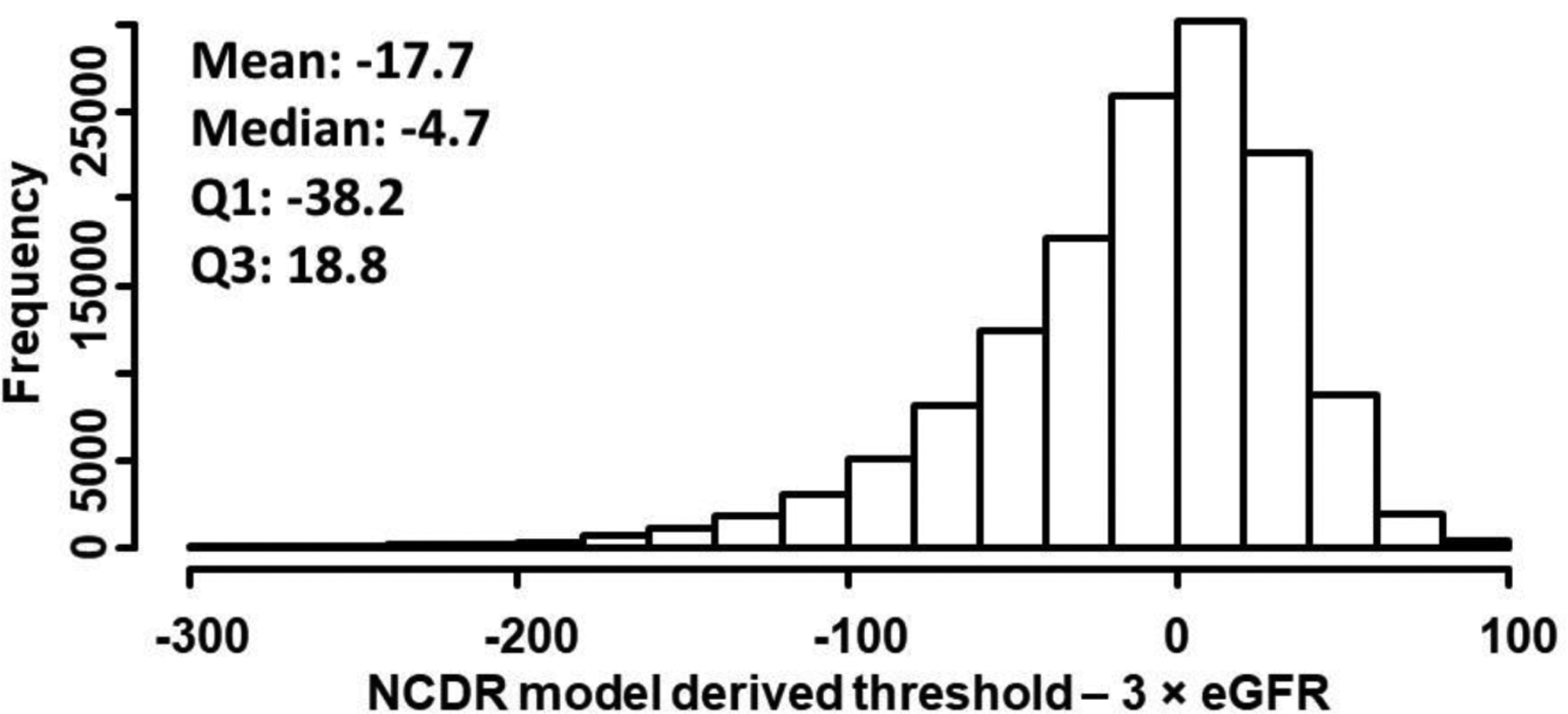
Background: Contrast volume used during percutaneous coronary intervention has a direct relationship with contrast-associated acute kidney injury. While several models estimate the risk of contrast-associated acute kidney injury, only the strategy of limiting contrast volume to 3 × estimated glomerular filtration rate (eGFR) gives actionable estimates of safe contrast volume doses. However, this method does not consider other patient characteristics associated with risk, such as age, diabetes or heart failure.
Methods: Using the National Cardiovascular Data Registry acute kidney injury risk model, we developed a novel strategy to define safe contrast limits by entering a contrast term into the model and using it to meet specific (eg, 10%) relative risk reductions. We then estimated acute kidney injury rates when our patient-centered model-derived thresholds were and were not exceeded using data from CathPCI version 5 between April 2018 and June 2019. We repeated the same analysis in a sub-set of patients who received ≤3 × eGFR contrast.
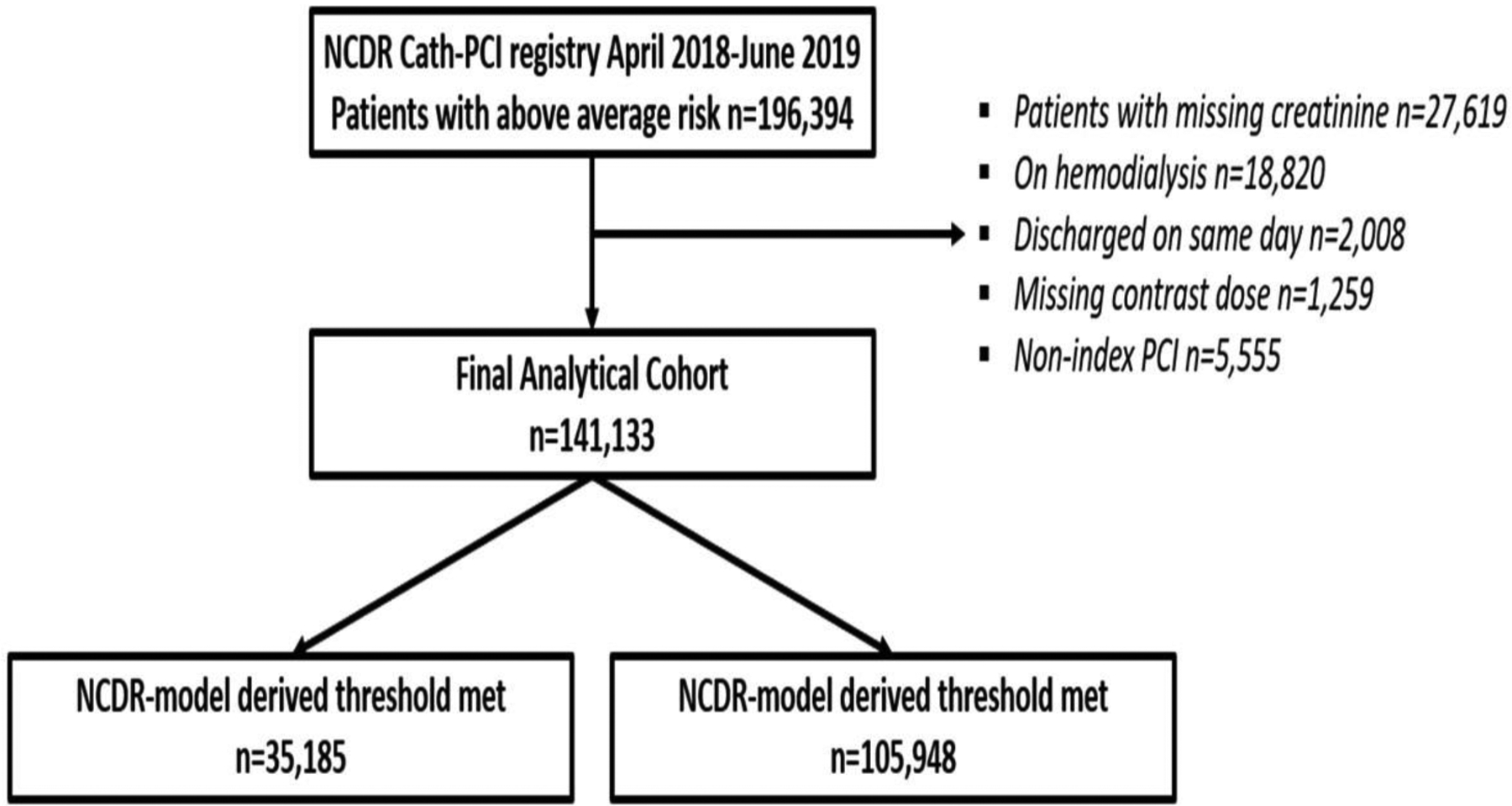
Results: After excluding patients on hemodialysis, below average risk (<7%), missing data and multiple percutaneous coronary interventions, our final analytical cohort included 141,133 patients at high risk for acute kidney injury. The rate of acute kidney injury was 10.0% when the contrast thresholds derived from our patient-centered model were met and 18.2% when they were exceeded (P < .001). In patients who received contrast ≤3 × eGFR (n = 82,318), contrast-associated acute kidney injury rate was 9.8% when the contrast thresholds derived from our patient centered model were met and 14.5% when they were exceeded (P < .001).
Conclusions: A novel strategy for developing personalized contrast volume thresholds, provides actionable information for providers that could decrease rates of contrast-associated acute kidney injury. This strategy needs further prospective testing to assess efficacy in improving patient outcomes.
Copyright © 2020 Elsevier Inc. All rights reserved.
Figures
References
-
- Chertow GM, Burdick E, Honour M, Bonventre JV, Bates DW. Acute kidney injury, mortality, length of stay, and costs in hospitalized patients. Journal of the American Society of Nephrology : JASN 2005;16:3365–70. - PubMed
-
- Gruberg L, Mehran R, Dangas G et al. Acute renal failure requiring dialysis after percutaneous coronary interventions. Catheterization and cardiovascular interventions : official journal of the Society for Cardiac Angiography & Interventions 2001;52:409–16. - PubMed
-
- Gupta R, Gurm HS, Bhatt DL, Chew DP, Ellis SG. Renal failure after percutaneous coronary intervention is associated with high mortality. Catheterization and cardiovascular interventions : official journal of the Society for Cardiac Angiography & Interventions 2005;64:442–8. - PubMed
-
- Subramanian S, Tumlin J, Bapat B, Zyczynski T. Economic burden of contrast-induced nephropathy: implications for prevention strategies. Journal of medical economics 2007;10:119–34. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
