

7T Epilepsy Task Force Consensus Recommendations on the Use of 7T MRI in Clinical Practice
- PMID: 33361257
- PMCID: PMC8055334
- DOI: 10.1212/WNL.0000000000011413
7T Epilepsy Task Force Consensus Recommendations on the Use of 7T MRI in Clinical Practice
Abstract
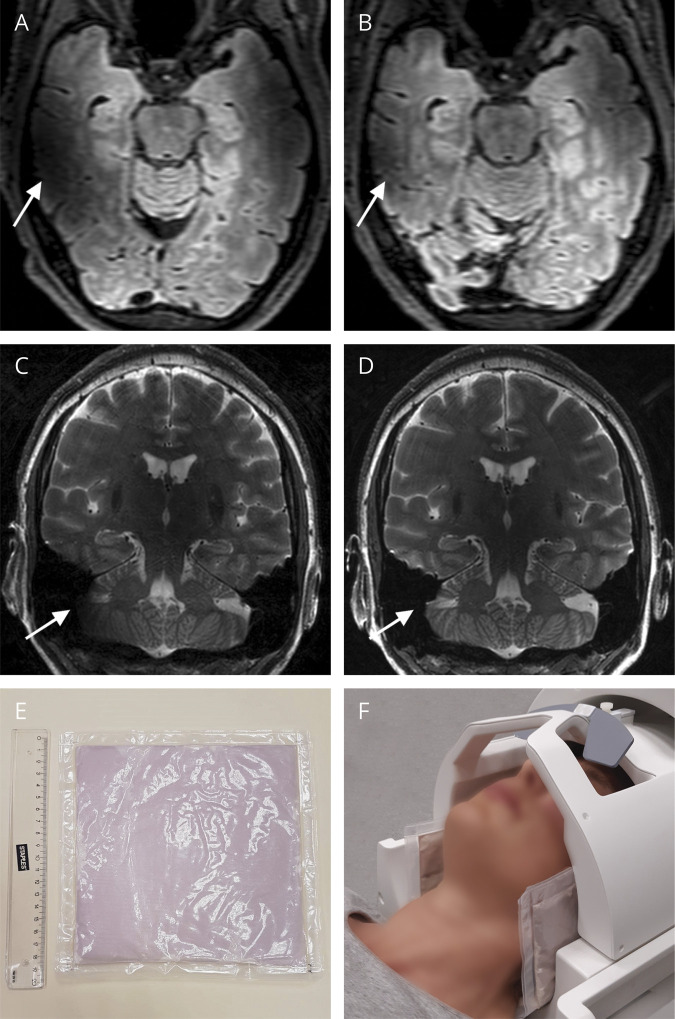
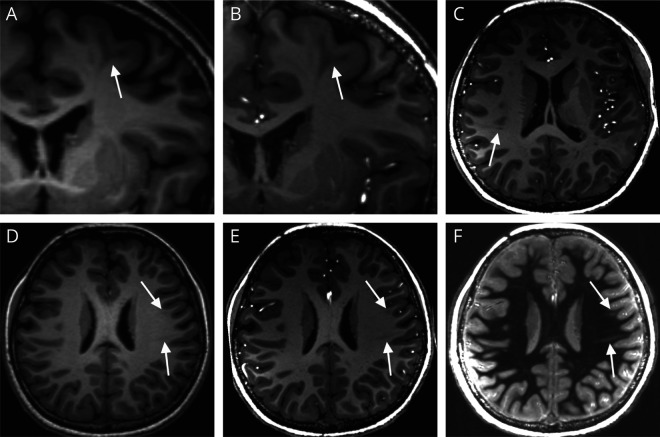
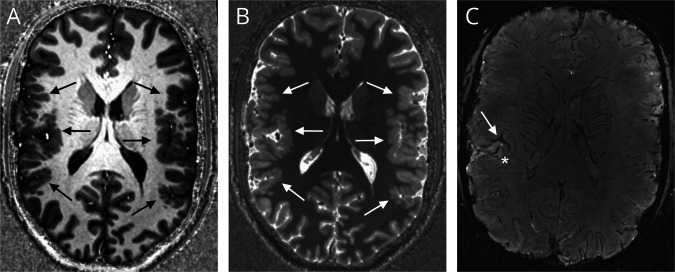
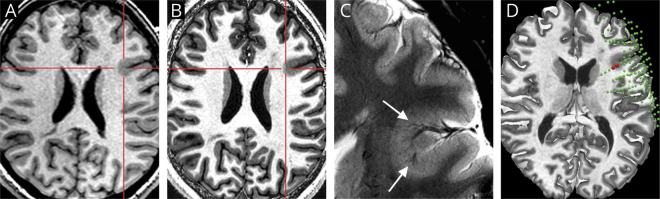
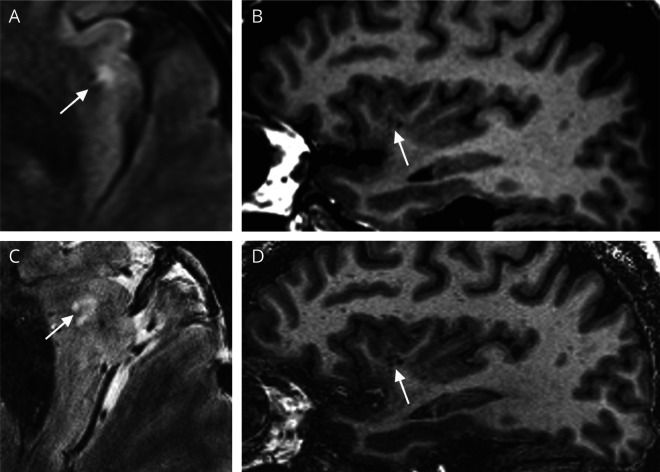
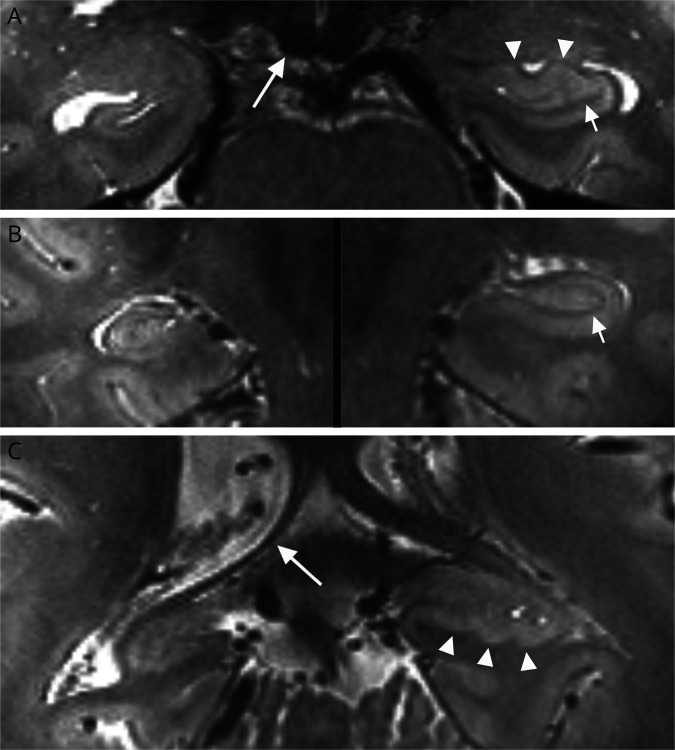
Identifying a structural brain lesion on MRI has important implications in epilepsy and is the most important factor that correlates with seizure freedom after surgery in patients with drug-resistant focal onset epilepsy. However, at conventional magnetic field strengths (1.5 and 3T), only approximately 60%-85% of MRI examinations reveal such lesions. Over the last decade, studies have demonstrated the added value of 7T MRI in patients with and without known epileptogenic lesions from 1.5 and/or 3T. However, translation of 7T MRI to clinical practice is still challenging, particularly in centers new to 7T, and there is a need for practical recommendations on targeted use of 7T MRI in the clinical management of patients with epilepsy. The 7T Epilepsy Task Force-an international group representing 21 7T MRI centers with experience from scanning over 2,000 patients with epilepsy-would hereby like to share its experience with the neurology community regarding the appropriate clinical indications, patient selection and preparation, acquisition protocols and setup, technical challenges, and radiologic guidelines for 7T MRI in patients with epilepsy. This article mainly addresses structural imaging; in addition, it presents multiple nonstructural MRI techniques that benefit from 7T and hold promise as future directions in epilepsy. Answering to the increased availability of 7T MRI as an approved tool for diagnostic purposes, this article aims to provide guidance on clinical 7T MRI epilepsy management by giving recommendations on referral, suitable 7T MRI protocols, and image interpretation.
© 2020 American Academy of Neurology.
Figures
References
-
- Ryvlin P, Cross JH, Rheims S. Epilepsy surgery in children and adults. Lancet Neurol 2014;13:1114–1126. - PubMed
-
- Téllez-Zenteno JF, Hernández Ronquillo L, Moien-Afshari F, Wiebe S. Surgical outcomes in lesional and non-lesional epilepsy: a systematic review and meta-analysis. Epilepsy Res 2010;89:310–318. - PubMed
-
- van der Zwaag W, Schäfer A, Marques JP, Turner R, Trampel R. Recent applications of UHF-MRI in the study of human brain function and structure: a review. NMR Biomed 2016;29:1274–1288. - PubMed
-
- Trattnig S, Bogner W, Gruber S, et al. Clinical applications at ultrahigh field (7 T). Where does it make the difference?. NMR Biomed 2016;29:1316–1334. - PubMed