

Automated Cerebral Hemorrhage Detection Using RAPID
- PMID: 33361378
- PMCID: PMC7872180
- DOI: 10.3174/ajnr.A6926
Automated Cerebral Hemorrhage Detection Using RAPID
Abstract
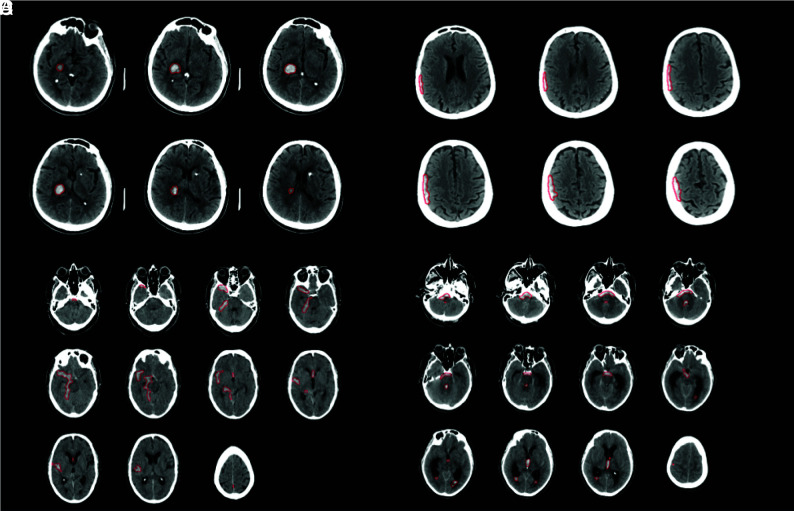
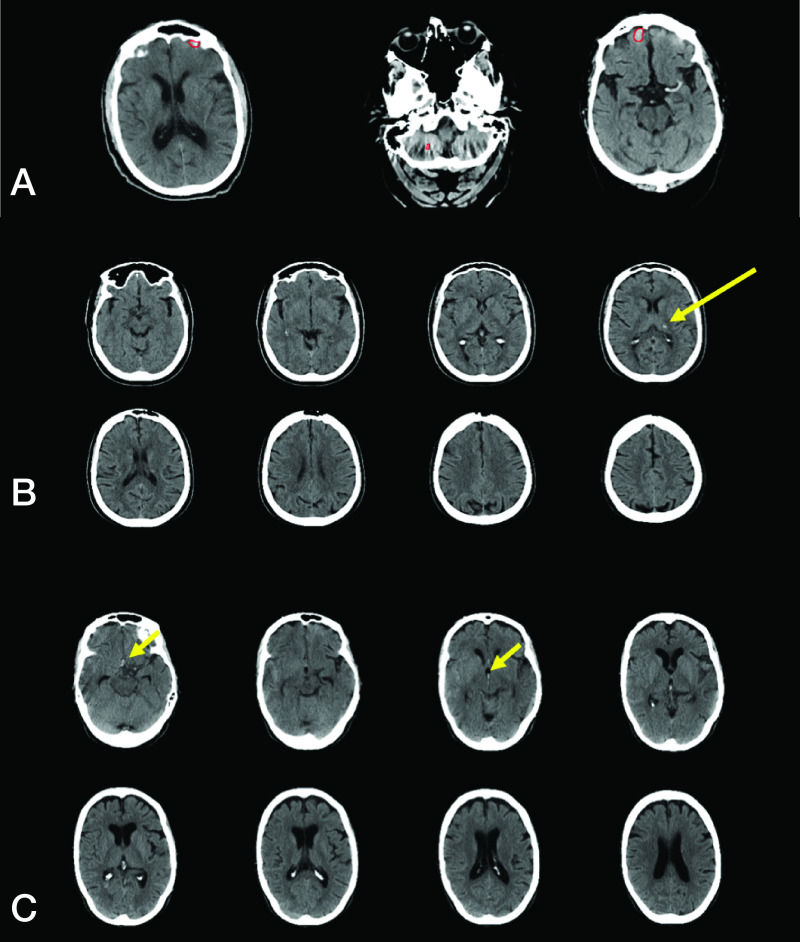
Background and purpose: Intracranial hemorrhage (ICH) is an important event that is diagnosed on head NCCT. Increased NCCT utilization in busy hospitals may limit timely identification of ICH. RAPID ICH is an automated hybrid 2D-3D convolutional neural network application designed to detect ICH that may allow for expedited ICH diagnosis. We determined the accuracy of RAPID ICH for ICH detection and ICH volumetric quantification on NCCT.
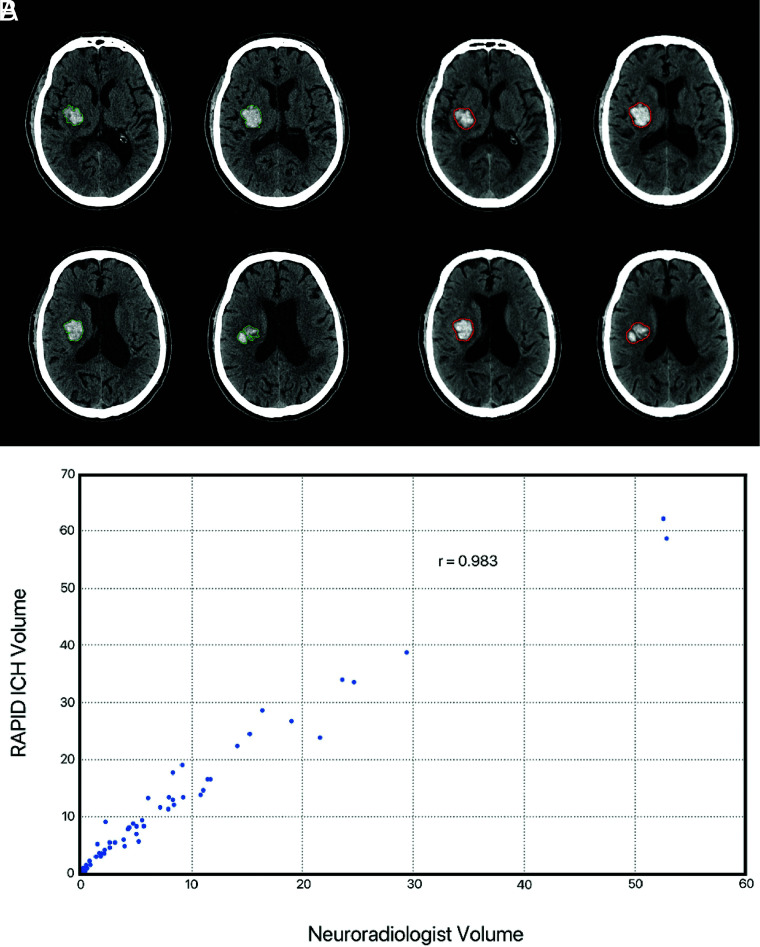
Materials and methods: NCCT scans were evaluated for ICH by RAPID ICH. Consensus detection of ICH by 3 neuroradiology experts was used as the criterion standard for RAPID ICH comparison. ICH volume was also automatically determined by RAPID ICH in patients with intraparenchymal or intraventricular hemorrhage and compared with manually segmented ICH volumes by a single neuroradiology expert. ICH detection accuracy, sensitivity, specificity, positive predictive value, negative predictive value, and positive and negative likelihood ratios by RAPID ICH were determined.
Results: We included 308 studies. RAPID ICH correctly identified 151/158 ICH cases and 143/150 ICH-negative cases, which resulted in high sensitivity (0.956, CI: 0.911-0.978), specificity (0.953, CI: 0.907-0.977), positive predictive value (0.956, CI: 0.911-0.978), and negative predictive value (0.953, CI: 0.907-0.977) for ICH detection. The positive likelihood ratio (20.479, CI 9.928-42.245) and negative likelihood ratio (0.046, CI 0.023-0.096) for ICH detection were similarly favorable. RAPID ICH volumetric quantification for intraparenchymal and intraventricular hemorrhages strongly correlated with expert manual segmentation (correlation coefficient r = 0.983); the median absolute error was 3 mL.
Conclusions: RAPID ICH is highly accurate in the detection of ICH and in the volumetric quantification of intraparenchymal and intraventricular hemorrhages.
© 2021 by American Journal of Neuroradiology.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical