

Diagnostic accuracy of magnetic resonance imaging for the detection of pulmonary nodules simulated in a dedicated porcine chest phantom
- PMID: 33362273
- PMCID: PMC7757901
- DOI: 10.1371/journal.pone.0244382
Diagnostic accuracy of magnetic resonance imaging for the detection of pulmonary nodules simulated in a dedicated porcine chest phantom
Abstract
Objective: CT serves as gold standard for the evaluation of pulmonary nodules. However, CT exposes patients to ionizing radiation, a concern especially in screening scenarios with repeated examinations. Due to recent technological advances, MRI emerges as a potential alternative for lung imaging using 3D steady state free precession and ultra-short echo-time sequences. Therefore, in this study we assessed the performance of three state-of-the-art MRI sequences for the evaluation of pulmonary nodules.
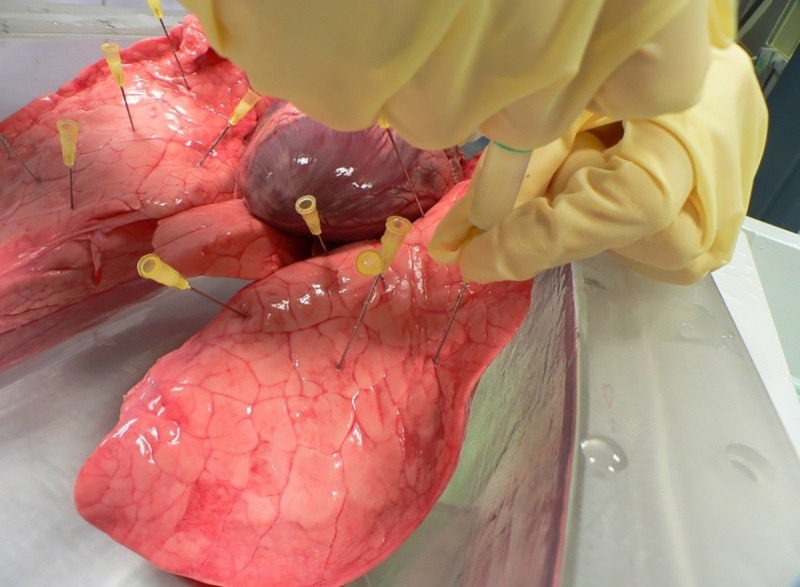
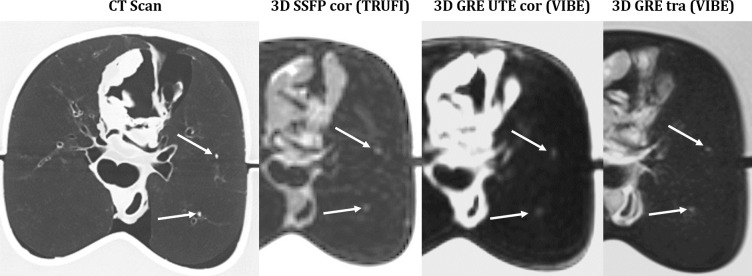
Methods: Lesions of variable sizes were simulated in porcine lungs placed in a dedicated chest phantom mimicking a human thorax, followed by CT and MRI examinations. Two blinded readers evaluated the acquired MR-images locating and measuring every suspect lesion. Using the CT-images as reference, logistic regression was performed to investigate the sensitivity of the tested MRI-sequences for the detection of pulmonary nodules.
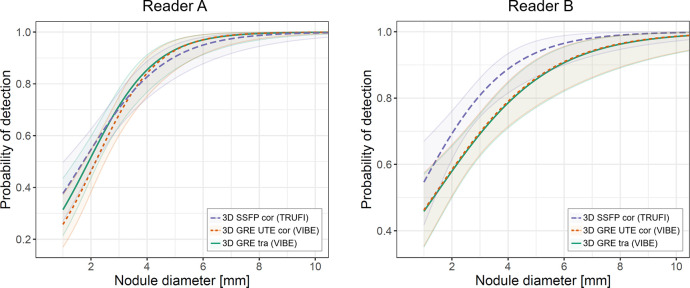
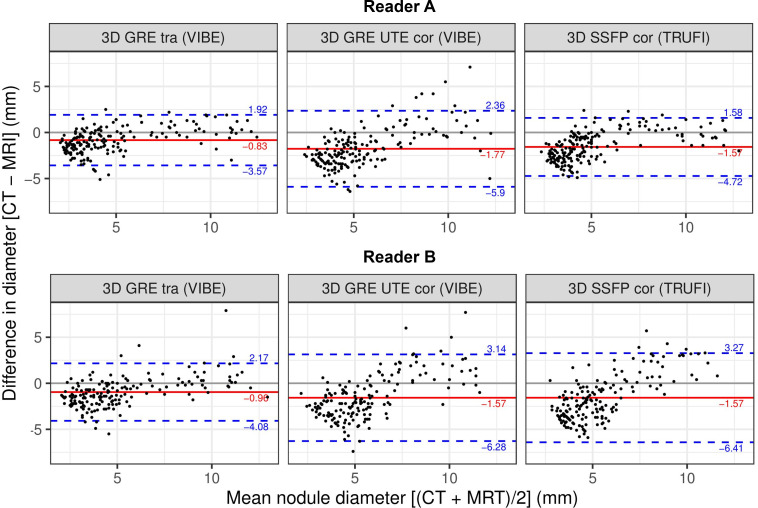
Results: For nodules with a diameter of 6 mm, all three sequences achieved high sensitivity values above 0.91. However, the sensitivity dropped for smaller nodules, yielding an average of 0.83 for lesions with 4 mm in diameter and less than 0.69 for lesions with 2 mm in diameter. The positive predictive values ranged between 0.91 and 0.96, indicating a low amount of false positive findings. Furthermore, the size measurements done on the MR-images were subject to a bias ranging from 0.83 mm to -1.77 mm with standard deviations ranging from 1.40 mm to 2.11 mm. There was no statistically significant difference between the three tested sequences.
Conclusion: While showing promising sensitivity values for lesions larger than 4 mm, MRI appears to be not yet suited for lung cancer screening. Nonetheless, the three tested MRI sequences yielded high positive predictive values and accurate size measurements; therefore, MRI could potentially figure as imaging method of the chest in selected follow-up scenarios, e.g. of incidental findings subject to the Fleischner Criteria.
Conflict of interest statement
Thomas Benkert is employed by Siemens Healthcare GmbH. We confirm that this does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
-
- Stewart BW, Wild CP, editors. World Cancer Report 2014. Lyon: International Agency for Research on Cancer/World Health Organization; 2014.
-
- Torre LA, Siegel RL, Jemal A. Lung Cancer Statistics In: Ahmad A, Gadgeel S, editors. Lung Cancer and Personalized Medicine [Internet]. Cham: Springer International Publishing; 2016. p. 1–19. 10.1007/978-3-319-24223-1_1. - DOI
-
- World Health Organization. The top 10 causes of death [Internet]. World Health Organization;2018. Available from: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death.
-
- IARC Working Group on the Evaluation of Carcinogenic Risk to Humans. Personal Habits and Indoor Combustions. Lyon: International Agency for Research on Cancer; 2012. (IARC Monographs on the Evaluation of Carcinogenic Risks to Humans. No. 100E). Available from: https://www.ncbi.nlm.nih.gov/books/NBK304391/. - PMC - PubMed
