

Robotic resection of liver focal nodal hyperplasia guided by indocyanine green fluorescence imaging: A preliminary analysis of 23 cases
- PMID: 33362911
- PMCID: PMC7739148
- DOI: 10.4251/wjgo.v12.i12.1407
Robotic resection of liver focal nodal hyperplasia guided by indocyanine green fluorescence imaging: A preliminary analysis of 23 cases
Abstract
Background: Focal nodal hyperplasia (FNH) is a common benign tumor of the liver. It occurs mostly in people aged 40-50 years and 90% of the patients are female. FNH can be cured by local resection. How to locate and judge the tumor boundary in real time is often a challenge for surgeons.
Aim: To summarize the technique and feasibility of robotic resection of FNH guided by indocyanine green (ICG) fluorescence imaging.
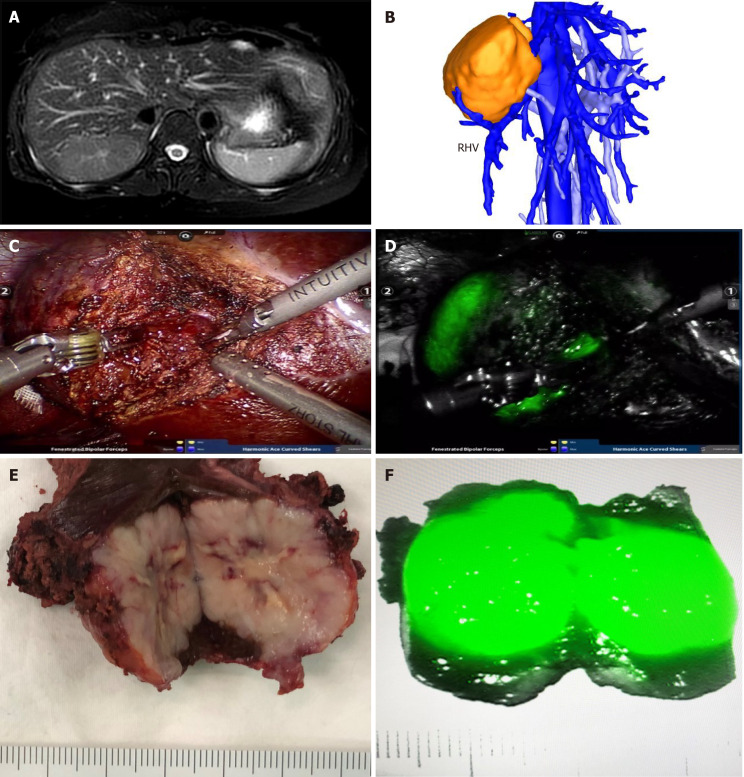
Methods: The demographics and perioperative outcomes of a consecutive series of patients who underwent robotic resection of liver FNH guided by ICG fluorescence imaging between May 1, 2018 and September 30, 2019 were retrospectively analyzed. ICG was injected through the median elbow vein in all the patients at a dose of 0.25 mg/kg 48 h before the operation. During the operation, the position of FNH in the liver was located in the fluorescence mode of the Da Vinci Si robot operating system and the tumor boundary was determined during the resection.
Results: Among the 23 patients, there were 11 males and 12 females, with a mean age of 30.5 ± 9.3 years. Twenty-two cases completed robotic resection, while one (4.3%) case converted to open surgery. In the robotic surgery group, the operation time was 35-340 min with a median of 120 min, the intraoperative bleeding was 10-800 mL with a median of 50 mL, and the postoperative hospital stay was 1-7 d with a median of 4 d. Biliary fistula occurred in two (8.7%) patients after robotic operation and they both recovered after conservative treatment. One (4.3%) patient received blood transfusion and there was no death in this study. The postoperative hospital stay in the small tumor group was significantly shorter than that in the large tumor group (P < 0.05).
Conclusion: ICG fluorescence imaging can guide the surgeon to perform robotic resection of liver FNH by locating the tumor and displaying the tumor boundary in real time. It is a safe and feasible method to ensure the complete resection of the tumor.
Keywords: Focal nodal hyperplasia; Hepatectomy; Indocyanine green; Robotic surgery.
©The Author(s) 2020. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors declare that they have no conflict of interest to disclose.
Figures
Similar articles
-
The Application of Indocyanine Green Fluorescence Imaging During Robotic Liver Resection: A Case-Matched Study.World J Surg. 2019 Oct;43(10):2595-2606. doi: 10.1007/s00268-019-05055-2. World J Surg. 2019. PMID: 31222642
-
Indocyanine green (ICG) fluorescent cholangiography during robotic cholecystectomy: results of 184 consecutive cases in a single institution.Surg Innov. 2014 Dec;21(6):615-21. doi: 10.1177/1553350614524839. Epub 2014 Mar 9. Surg Innov. 2014. PMID: 24616013
-
Deploying Indocyanine Green Fluorescence-Guided Navigation System in Precise Laparoscopic Resection of Pediatric Hepatoblastoma.Cancers (Basel). 2022 Dec 9;14(24):6057. doi: 10.3390/cancers14246057. Cancers (Basel). 2022. PMID: 36551543 Free PMC article.
-
Robotic single-site endometriosis resection using near-infrared fluorescence imaging with indocyanine green: a prospective case series and review of literature.J Robot Surg. 2020 Feb;14(1):145-154. doi: 10.1007/s11701-019-00951-0. Epub 2019 Apr 1. J Robot Surg. 2020. PMID: 30937836 Review.
-
Does application of indocyanine green fluorescence imaging enhance clinical outcomes in liver resection? A meta-analysis.Photodiagnosis Photodyn Ther. 2021 Dec;36:102554. doi: 10.1016/j.pdpdt.2021.102554. Epub 2021 Sep 28. Photodiagnosis Photodyn Ther. 2021. PMID: 34597831 Review.
Cited by
-
Augmented Reality and Image-Guided Robotic Liver Surgery.Cancers (Basel). 2021 Dec 14;13(24):6268. doi: 10.3390/cancers13246268. Cancers (Basel). 2021. PMID: 34944887 Free PMC article. Review.
-
Application of indocyanine green fluorescence imaging in hepatobiliary surgery.Int J Surg. 2024 Dec 1;110(12):7948-7961. doi: 10.1097/JS9.0000000000001802. Int J Surg. 2024. PMID: 38884267 Free PMC article. Review.
-
Real-Time Navigation in Liver Surgery Through Indocyanine Green Fluorescence: An Updated Analysis of Worldwide Protocols and Applications.Cancers (Basel). 2025 Mar 3;17(5):872. doi: 10.3390/cancers17050872. Cancers (Basel). 2025. PMID: 40075718 Free PMC article. Review.
-
The Role of ICG in Robot-Assisted Liver Resections.J Clin Med. 2022 Jun 19;11(12):3527. doi: 10.3390/jcm11123527. J Clin Med. 2022. PMID: 35743595 Free PMC article.
-
Surgical margin status outcome of intraoperative indocyanine green fluorescence-guided laparoscopic hepatectomy in liver malignancy: a systematic review and meta-analysis.BMC Surg. 2024 Jun 12;24(1):181. doi: 10.1186/s12893-024-02469-1. BMC Surg. 2024. PMID: 38867212 Free PMC article.
References
-
- Gürses C, Okşar FS, Erol B, Yalçın M, Kahvecioğlu N, Alparslan AŞ. Natural course of hepatic focal nodular hyperplasia from childhood to adulthood and review of the literature. Turk J Gastroenterol. 2017;28:492–497. - PubMed
-
- Matsukuma KE, Yeh MM. Update on the pathology of liver neoplasms. Ann Diagn Pathol. 2019;38:126–137. - PubMed
-
- Giambelluca D, Taibbi A, Midiri M, Bartolotta TV. The "spoke wheel" sign in hepatic focal nodular hyperplasia. Abdom Radiol . 44:1183–1184. - PubMed
-
- van Rosmalen BV, de Graeff JJ, van der Poel MJ, de Man IE, Besselink M, Abu Hilal M, Busch OR, Verheij J, van Gulik TM Dutch Benign Liver Tumour Group. Impact of open and minimally invasive resection of symptomatic solid benign liver tumours on symptoms and quality of life: a systematic review. HPB . 21:1119–1130. - PubMed
LinkOut - more resources
Full Text Sources
