

Outcomes of neoadjuvant chemoradiotherapy followed by radical resection for T4 colorectal cancer
- PMID: 33362913
- PMCID: PMC7739149
- DOI: 10.4251/wjgo.v12.i12.1428
Outcomes of neoadjuvant chemoradiotherapy followed by radical resection for T4 colorectal cancer
Abstract
Background: Patients with clinical T4 colorectal cancer (CRC) have a poor prognosis because of compromised surgical margins. Neoadjuvant therapy may be effective in downstaging tumors, thereby rendering possible radical resection with clear margins.
Aim: To evaluate tumor downsizing and resection with clear margins in T4 CRC patients undergoing neoadjuvant concurrent chemoradiotherapy followed by surgery.
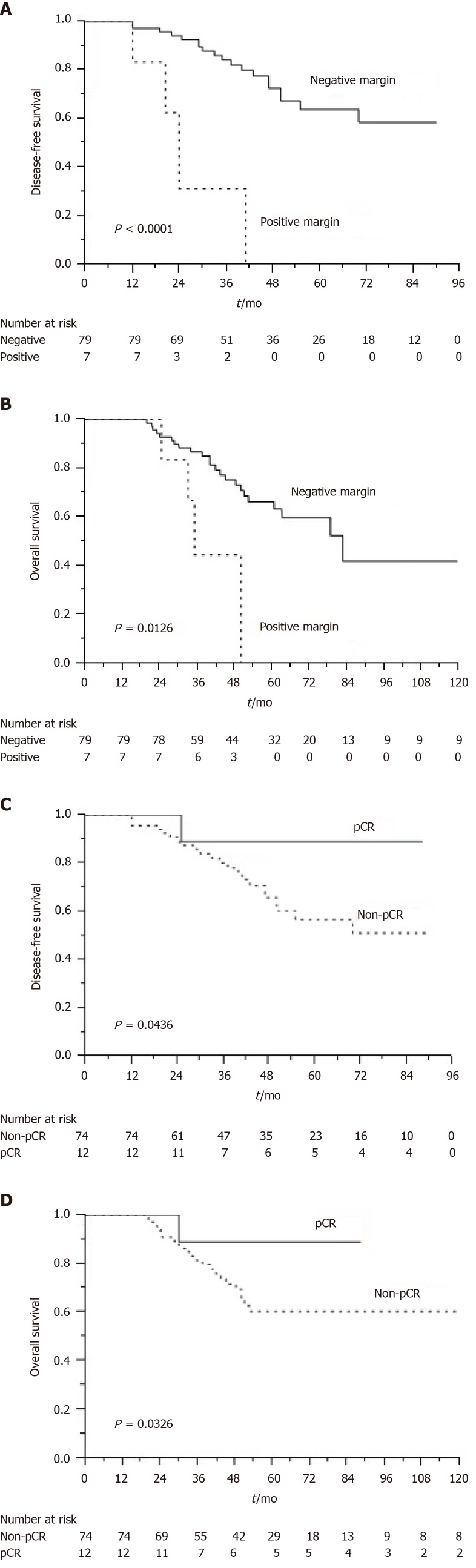
Methods: This study retrospectively included 86 eligible patients with clinical T4 CRC who underwent neoadjuvant concurrent chemoradiotherapy followed by radical resection. Neoadjuvant therapy consisted of radiation therapy at a dose of 45-50.4 Gy and chemotherapy agents, either FOLFOX or capecitabine. A circumferential resection margin (CRM) of < 1 mm was considered to be a positive margin. We defined pathological complete response (pCR) as the absence of any malignant cells in a specimen, including the primary tumor and lymph nodes. A multivariate logistic regression model was used to identify independent predictive factors for pCR.
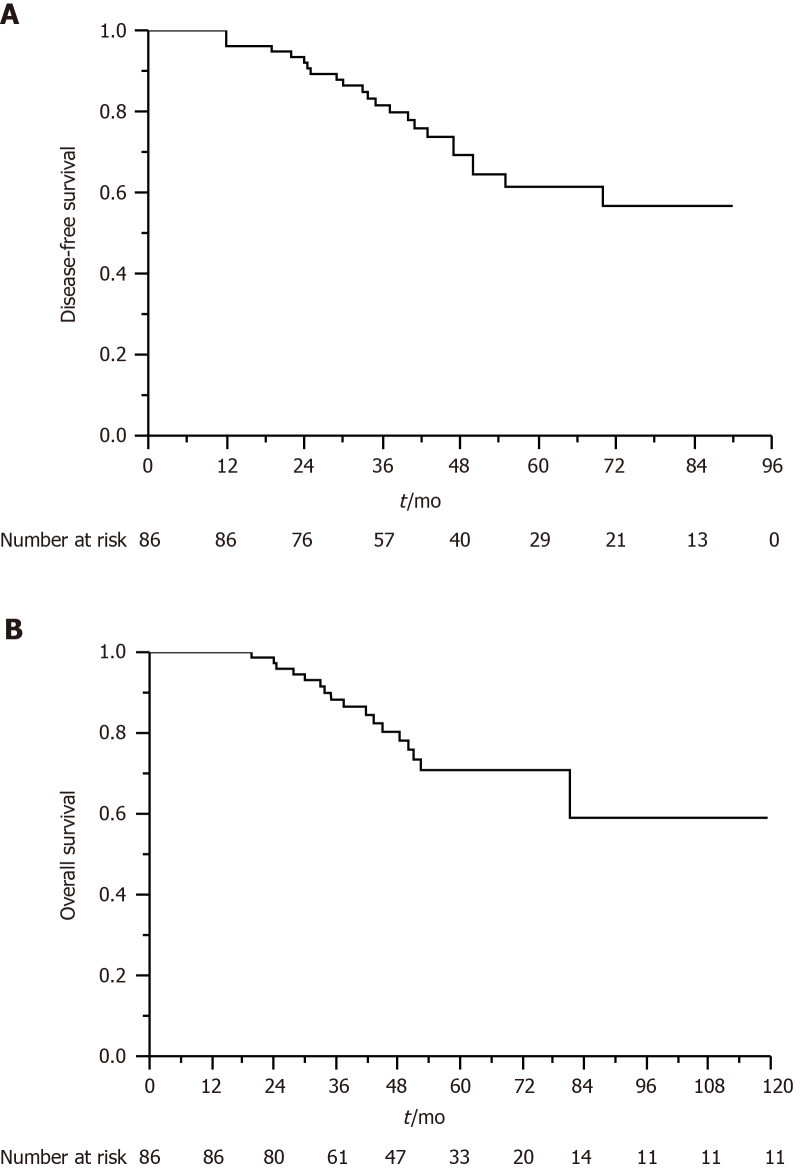
Results: For 86 patients who underwent neoadjuvant chemoradiotherapy and surgery, the rate of pCR was 14%, and the R0 resection rate was 91.9%. Of the 61 patients with rectal cancer, 7 (11.5%) achieved pCR and 5 (8.2%) had positive CRMs. Of the 25 patients with colon cancer, 5 (20%) achieved pCR and 2 (8%) had positive CRMs. We observed that the FOLFOX regimen was an independent predictor of pCR (P = 0.046). After a median follow-up of 47 mo, the estimated 5-year overall survival (OS) and disease-free survival (DFS) rates were 70.8% and 61.4%, respectively. Multivariate analysis revealed that a tumor with a negative resection margin was associated with improved DFS (P = 0.014) and OS (P = 0.001). Patients who achieved pCR exhibited longer DFS (P = 0.042) and OS (P = 0.003) than those who did not.
Conclusion: Neoadjuvant concurrent chemoradiotherapy engenders favorable pCR and R0 resection rates among patients with T4 CRC. The R0 resection rate and pCR are independent prognostic factors for patients with T4 CRC.
Keywords: Chemoradiotherapy; Colorectal cancer; Pathological complete response; R0 resection; Survival; T4.
©The Author(s) 2020. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors declare that they have no conflicts of interest to disclose.
Figures
Similar articles
-
Prognostic value of the circumferential resection margin and its definitions in esophageal cancer patients after neoadjuvant chemoradiotherapy.Dis Esophagus. 2018 Feb 1;31(2). doi: 10.1093/dote/dox117. Dis Esophagus. 2018. PMID: 29036407
-
Induction chemotherapy improved outcomes of patients with resectable esophageal cancer who received chemoradiotherapy followed by surgery.Int J Radiat Oncol Biol Phys. 2004 Oct 1;60(2):427-36. doi: 10.1016/j.ijrobp.2004.03.033. Int J Radiat Oncol Biol Phys. 2004. PMID: 15380576
-
[Neoadjuvant chemoradiotherapy combined with surgery versus direct surgery in the treatment of Siewert type II and III adenocarcinomas of the esophagogastric junction: long-term prognostic analysis of a prospective randomized controlled trial].Zhonghua Wei Chang Wai Ke Za Zhi. 2021 Feb 25;24(2):128-137. doi: 10.3760/cma.j.cn.441530-20201019-00565. Zhonghua Wei Chang Wai Ke Za Zhi. 2021. PMID: 33508918 Clinical Trial. Chinese.
-
Interventions and Outcomes for Neoadjuvant Treatment of T4 Colon Cancer: A Scoping Review.Curr Oncol. 2021 May 29;28(3):2065-2078. doi: 10.3390/curroncol28030191. Curr Oncol. 2021. PMID: 34072615 Free PMC article.
-
Neoadjuvant therapy versus direct to surgery for T4 colon cancer: meta-analysis.Br J Surg. 2021 Dec 17;109(1):30-36. doi: 10.1093/bjs/znab382. Br J Surg. 2021. PMID: 34921604
Cited by
-
Critical reappraisal of neoadjuvant concurrent chemoradiotherapy for treatment of locally advanced colon cancer.PLoS One. 2021 Nov 2;16(11):e0259460. doi: 10.1371/journal.pone.0259460. eCollection 2021. PLoS One. 2021. PMID: 34727133 Free PMC article.
-
Preoperative radiotherapy does not improve and may even be detrimental to the long-term prognosis of patients diagnosed with stage III colon adenocarcinoma: a propensity score-matched SEER database analysis.Front Oncol. 2023 Nov 22;13:1324485. doi: 10.3389/fonc.2023.1324485. eCollection 2023. Front Oncol. 2023. PMID: 38074673 Free PMC article.
-
Narrative review of neoadjuvant therapy in patients with locally advanced colon cancer.Kaohsiung J Med Sci. 2025 Feb;41(2):e12926. doi: 10.1002/kjm2.12926. Epub 2024 Dec 24. Kaohsiung J Med Sci. 2025. PMID: 39717937 Free PMC article. Review.
-
Outcomes of neoadjuvant chemoradiotherapy in T4 rectal cancer patients: a real-world single institution experience.Radiat Oncol J. 2024 Dec;42(4):273-280. doi: 10.3857/roj.2024.00136. Epub 2024 Sep 19. Radiat Oncol J. 2024. PMID: 39748528 Free PMC article.
-
Predictive Value of the Interaction between CEA and Hemoglobin in Neoadjuvant CCRT Outcomes in Rectal Cancer Patients.J Clin Med. 2023 Dec 14;12(24):7690. doi: 10.3390/jcm12247690. J Clin Med. 2023. PMID: 38137759 Free PMC article.
References
-
- Siegel R, Desantis C, Jemal A. Colorectal cancer statistics, 2014. CA Cancer J Clin . 2014;64:104–117. - PubMed
-
- Ministry of Health and Welfare, the Executive Yuan, Republic of China. Health and Vital Statistics. Available from: http://www.mohw.gov.tw/CHT/Ministry/
-
- Ueno H, Mochizuki H, Akagi Y, Kusumi T, Yamada K, Ikegami M, Kawachi H, Kameoka S, Ohkura Y, Masaki T, Kushima R, Takahashi K, Ajioka Y, Hase K, Ochiai A, Wada R, Iwaya K, Shimazaki H, Nakamura T, Sugihara K. Optimal colorectal cancer staging criteria in TNM classification. J Clin Oncol . 2012;30:1519–1526. - PubMed
LinkOut - more resources
Full Text Sources
